IN A NUTSHELL Editor's noteIn this article, the Author takes into account the results from a new study, published in The Lancet, funded by the Bill & Melinda Gates Foundation, which emphasizes the importance of considering sex and gender differences in health outcomes, while facing Health Inequity that weakens the value of Public Health. As the Author maintains, ‘to dismantle the systemic barriers perpetuating gender inequities in health, we must adopt a multifaceted approach that includes sub-national analysis as a critical tool’. In such an endeavour, investing in data, empowering communities, building capacity, reforming policies and challenging norms must serve as not to be given up pillars.

By Philip J Gover BA MA MPH
Public Health Consultant, Cooperation Works
Unmasking Gender Inequities in Health: Research Findings & A Roadmap to Gender-Equitable UHC
Universal Health Coverage (UHC), a global health goal introduced by the World Health Organization (WHO), aims to ensure equitable access to essential health services without financial barriers. Its significance lies in its potential to enhance health outcomes, reduce inequalities, and foster economic development. UHC offers several benefits, including access to essential medical services, improved health outcomes, mitigation of health disparities, and promotion of economic growth.
Achieving UHC presents challenges across all economies, particularly in low-income countries. Structural barriers such as high healthcare costs, disparities in insurance coverage, and limited healthcare availability hinder access to care. However, recent research[1] published in The Lancet, funded by the Bill & Melinda Gates Foundation, highlights the importance of considering sex and gender differences in health outcomes, adding further complexity to the planning and delivery of UHC.
Key Insights from Research
The research article provides several key insights regarding health differences between females and males across different age groups and geographies. Key insights and conclusions from the research include:
Global Health Disparities: The study reveals substantial global health differences between females and males, with little progress in bridging these disparities from 1990 to 2021. Conditions such as depressive disorders, anxiety disorders, and road injuries disproportionately affect females or males, with disparities emerging as early as adolescence and continuing to grow over the life course.
Regional Patterns: The research highlights various regional patterns in the distribution of disease burden across age groups for females and males. Variations in the prevalence of different health conditions across regions underscore the complex and context-specific relationships between health and gender norms, economic conditions, and social practices.
Importance of Gender-Sensitive Interventions: The findings underscore the importance of developing gender-sensitive interventions and preventive measures from a young age to address growing health differences between females and males across life stages. Gender norms and attitudes intensify during adolescence, emphasizing the need for early interventions that consider social determinants of health.
In addition to gender, it is crucial to recognize the intersecting influences of race, ethnicity, socioeconomic status, and geographical location on health outcomes. Intersectionality underscores the complex interplay between various social determinants of health, magnifying disparities experienced by marginalized communities. For instance, women of colour may face compounded barriers to accessing healthcare due to systemic racism and economic inequality. Similarly, rural communities may encounter distinct health challenges stemming from limited healthcare infrastructure and resources. By adopting an intersectional lens, policymakers and healthcare providers can develop more targeted interventions that address the unique needs of diverse populations, thereby advancing health equity.
Need for Inclusive Health Data: The study highlights the need for inclusive health data that span the gender spectrum to support more comprehensive and equitable health research. Current data limitations, including the binary framework of female or male in data disaggregation, hinder the analysis of health differences for gender-diverse individuals.
Persistent Health Differences: Despite advancements in understanding sex and gender disparities in health, the research underscores the persistent nature of health differences between females and males. The study calls for continued innovation in analysing health data from a gender perspective to address the roots of health disparities and promote health equity.
Life Course Approach: The research emphasizes the importance of adopting a life course approach in strategic planning for health systems to address the diverse and evolving health needs of females and males across different life stages. Effective health system strategies should consider the interplay between sex, gender, and other social determinants of health.
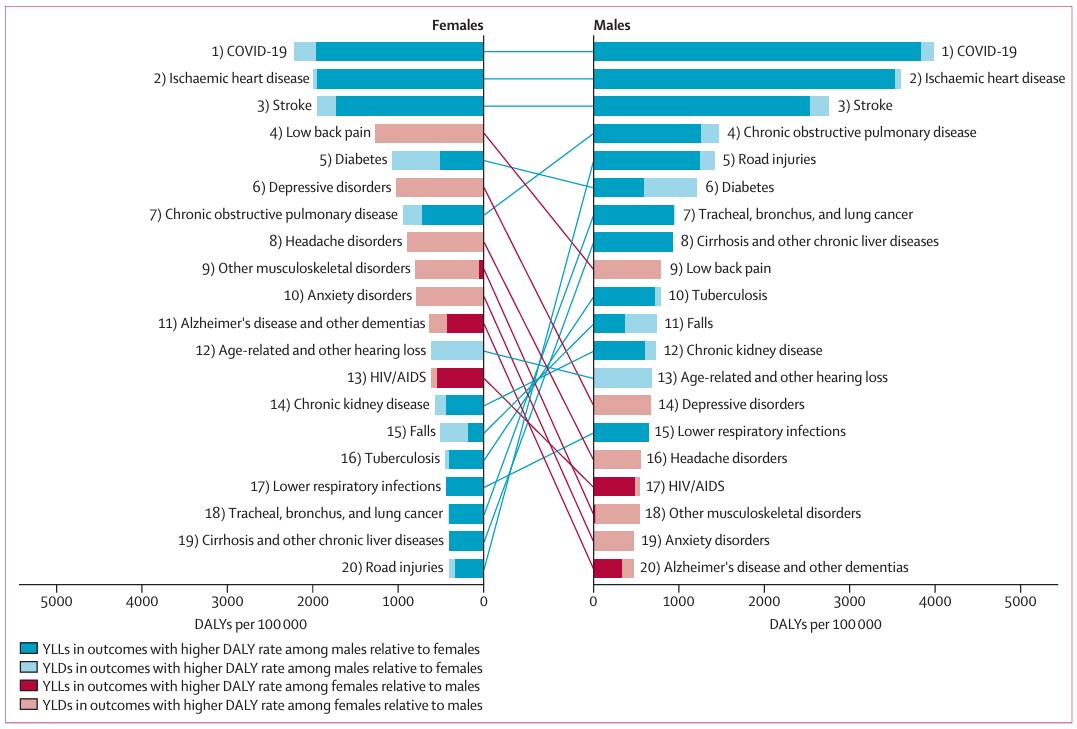
[Figure 1 – Global rankings of the top 20 causes of DALYs globally for females and males, age-standardised (10 years and older), 2021]
The list of causes of disease burden represents the top 20 causes of age-standardised DALYs observed across females and males for the age group of 10 years and older globally in 2021. This same list of health conditions was ranked according to the DALY rates (per 100 000 population) for both females and males globally in 2021 for the same age group. The colours of the bars and lines denote whether DALY rates are higher for females (red) or males (blue) as established by whether the 95% uncertainty interval of the absolute difference in DALY rates includes zero. The degree of transparency reflects the composition of DALYs for each cause, split between mortality (YLL) and morbidity (YLD). DALY=disability-adjusted life-year. YLL=years of life lost. YLD=years lived with disability.
In conclusion, the research article highlights the ongoing health disparities between females and males globally, the regional variations in disease burden, the importance of gender-sensitive interventions, the need for inclusive health data, and the significance of adopting a life course approach in healthcare planning to promote health equity and address health differences across diverse populations.
Limitations and Considerations
Acknowledging several limitations, including the inability to fully disentangle the influences of sex and gender on health outcomes, the study calls for more inclusive health research that considers intersectionality with other determinants of health.
The research emphasizes the necessity of adopting sex-informed and gender-informed strategies to address the distinct health challenges faced by men and women at different stages of life. This approach is crucial for achieving an equitable and healthy future for all individuals. Additionally, incorporating a sub-national perspective into these strategies can ensure that interventions are tailored to the specific needs of different regions and populations.
The research also hints at the need for sub-national analysis to understand how these disparities manifest at a local level. By examining data at a sub-national level, researchers can identify localized health challenges, tailor interventions to specific regions, and allocate resources effectively to address disparities within different communities.
While national-level data provides a crucial overview of gender disparities in health, sub-national analysis offers a more granular understanding of these inequities. By examining health outcomes at the district or community level, policymakers and healthcare providers can identify localized challenges and tailor interventions to specific populations. This approach has proven successful in addressing other health disparities, such as maternal mortality and infectious disease outbreaks. For example, in India, sub-national analysis revealed significant variations in maternal mortality rates across states, prompting targeted interventions that led to a substantial decline in overall maternal deaths. Similarly, in Cambodia, sub-national data has been used to identify high-risk areas for malaria transmission, allowing for targeted distribution of bed nets and antimalarial medications. These examples demonstrate the potential of sub-national analysis to inform effective and equitable healthcare strategies, particularly in addressing the complex issue of gender disparities in health.
The Cambodian Context
In Cambodia, the unique burden of disease, that represents its top 20 causes of age-standardised DALYs will be slightly different from that of the global collection. However, the underlying research illustrates that without assessment, gender-based access can be inhibited. This is important for economies like Cambodia, as addressing its health inequities requires a nuanced understanding of various demographic factors and gender dynamics that play a crucial and influential role in the provision of healthcare.
The female population outnumbers males by 2-4%. This demographic skew is further compounded by a pattern of rural to urban migration, whereby men predominantly leave provincial districts for city-based employment opportunities, leaving behind a disproportionately female rural population. Beyond this, it is asserted that there are still a significant number of rural communities, within localities, still unmapped.[2]
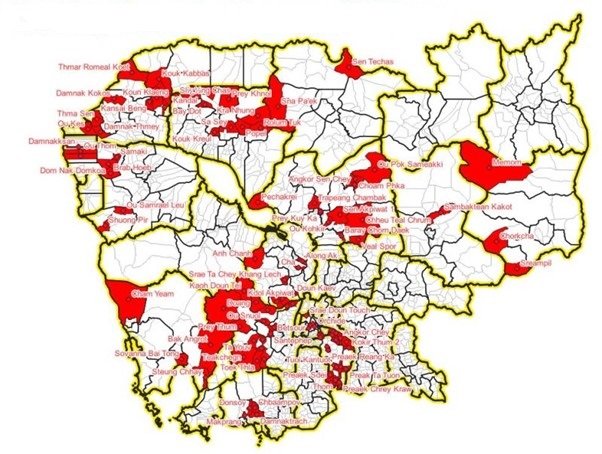
[Figure 2 – Unmapped Villages and Towns in Cambodia, 2019]
Women, in general, also tend to outlive men both locally and globally, resulting in an aging and rural population, predominantly comprised of older women. Adding further complexity is the consideration associated with the healthcare needs of prisoners, especially those of older incarcerated men and women, living out their lives in settings, where healthcare standards inside the prison gate fall way short of the limited standards that already exist outside the gate.
Sub-National Analysis: A Critical Tool for Action
Policymakers are increasingly recognizing the value of sub-national and sub-regional analysis in healthcare. By collecting and analysing health data within districts or communities, typically organized into cohorts of around 100,000 individuals (100k Analysis), we can identify regional and often sub-regional disparities in health outcomes, healthcare access, and resource allocation. This approach enables policymakers and healthcare providers to gain insights into localized health needs, prioritize interventions, and allocate resources more effectively.
The 100k Analysis approach can help facilitate a focus that examines and unmasks the granular detail of health outcomes, disparities, and healthcare utilization patterns within specific geographic areas.
While sub-national analysis offers a promising avenue for addressing gender inequities in health, it is important to acknowledge the potential challenges and limitations of this approach. Data availability and quality can vary significantly across regions, particularly in resource-limited settings. Additionally, financial and human resource constraints may hinder the implementation of comprehensive sub-national analysis. Strong political will and coordination among various stakeholders are essential for success, but can be challenging to achieve. Furthermore, the complexity of health systems and the interplay of multiple factors beyond gender may not be fully captured by sub-national analysis alone. Finally, equity considerations must be prioritized to ensure that resources and interventions are distributed fairly across all populations.
While challenges exist in capturing the complex nature of health needs within a fixed population size, the benefits of this approach outweigh the drawbacks. By complementing population-based analyses with localized evaluations, we can develop targeted interventions that address the diverse and evolving health needs of rural and urban populations across different age groups.
A Roadmap to Gender-Equitable UHC
To dismantle the systemic barriers perpetuating gender inequities in health, we must adopt a multifaceted approach that includes sub-national analysis as a critical tool:
- Invest in Data: We need robust, sex-disaggregated data at both national and sub-national levels. This data must inform targeted interventions and policies addressing the specific health needs of different populations in different regions.
- Empower Communities: Engage with communities at all levels, especially marginalized groups, to raise awareness of gender disparities and empower them to advocate for their health rights.
- Build Capacity: Provide healthcare professionals with training and resources to deliver gender-sensitive care free from bias and discrimination, ensuring that this capacity is distributed equitably across regions.
- Reform Policies: Advocate for policies promoting gender equity in all aspects of health, from access to services to research funding, with consideration for regional variations in health needs.
- Challenge Norms: Confront harmful social norms and power dynamics that drive gender disparities in health, recognizing that these norms can vary across different communities and regions.
The time for action is now. By working together, we can create a world where all individuals, regardless of gender or geography, have the opportunity to live healthy, fulfilling lives. This is not just a matter of justice; it is an investment in the future of our societies. When we prioritize gender equity and sub-national analysis in health, we create a ripple effect of positive change that extends to all aspects of life.
Author profile Philip J Gover BA MA MPH Public Health Consultant based in Cambodia with Cooperation.Works Mobile and open to program and research management opportunities that address inequalities in Public Health, Social Justice and Sustainable Development. I solve complex development challenges, designing innovative programs and securing funding through strategic partnerships. With a proven track record in Community Development, Public Health, and Business Enterprise, I like to drive projects from concept to implementation. Passionate about the UN SDGs, I aim to support and empower communities to create sustainable solutions. I enjoy coaching teams and mentoring talent and I take calculated risks to achieve transformative change. Let's connect if you seek a change-maker with vision and execution. philip.gover@cooperation.works https://www.linkedin.com/in/pjgover
References
[1] Patwardhan, V., Gil, G. F., Arrieta, A., Cagney, J., DeGraw, E., Herbert, M. E., … & Flor, L. S. (2024). Differences across the lifespan between females and males in the top 20 causes of disease burden globally: a systematic analysis of the Global Burden of Disease Study 2021. The Lancet Public Health, 9(5), e282-e294. Available here
By the same Author on PEAH Who Suffers Most: The Visibility of Children and Older People in Prison Diversionary Measures for Children in Conflict with the Law Reaching out and Engaging with SE Asian Communities: Health, Shared Value and Business