IN A NUTSHELL
Authors' Note
 Background: Unsafe abortion is a leading cause of maternal morbidity and mortality, particularly among vulnerable populations such as female sex workers (FCSWs). In Uganda, little is known about the prevalence and determinants of abortion-related health risks in this population, especially in rural districts like Kyotera. This study aimed to assess the factors associated with abortion-related health risks among FCSWs in Kyotera District, Uganda.
Methods: A cross-sectional study was conducted among 152 FSWs in Kyotera District. Participants were recruited using purposive and snowball sampling. Data were collected via structured questionnaires and key informant interviews. Quantitative data were analyzed using SPSS v26 with descriptive statistics and logistic regression to identify factors associated with abortion-related health risks. Qualitative data were analyzed thematically to supplement quantitative findings.
Results: Overall, 49% experienced abortion-related health risks and nearly half (48.7%) of participants reported a history of abortion, with 37% experiencing complications and 70.3% undergoing unsafe procedures. Significant predictors of abortion-related health risks included awareness of safe abortion services (Exp(B)=0.29, 95% CI: 0.11-0.79, p=0.018), access to post-abortion care, (Exp(B)=0.40, 95% CI: 0.18-0.89, p=0.026), and satisfaction with SRHS (Exp(B)=0.32, 95% CI: 0.13-0.79, p=0.013).
Conclusion: FCSWs in Kyotera District face a high burden of abortion-related health risks. Targeted interventions addressing SRHS (sexual and reproductive health services) access, stigma, and healthcare provider attitudes are crucial to reducing abortion-related complications.
Link to the original dissertation HERE
Background: Unsafe abortion is a leading cause of maternal morbidity and mortality, particularly among vulnerable populations such as female sex workers (FCSWs). In Uganda, little is known about the prevalence and determinants of abortion-related health risks in this population, especially in rural districts like Kyotera. This study aimed to assess the factors associated with abortion-related health risks among FCSWs in Kyotera District, Uganda.
Methods: A cross-sectional study was conducted among 152 FSWs in Kyotera District. Participants were recruited using purposive and snowball sampling. Data were collected via structured questionnaires and key informant interviews. Quantitative data were analyzed using SPSS v26 with descriptive statistics and logistic regression to identify factors associated with abortion-related health risks. Qualitative data were analyzed thematically to supplement quantitative findings.
Results: Overall, 49% experienced abortion-related health risks and nearly half (48.7%) of participants reported a history of abortion, with 37% experiencing complications and 70.3% undergoing unsafe procedures. Significant predictors of abortion-related health risks included awareness of safe abortion services (Exp(B)=0.29, 95% CI: 0.11-0.79, p=0.018), access to post-abortion care, (Exp(B)=0.40, 95% CI: 0.18-0.89, p=0.026), and satisfaction with SRHS (Exp(B)=0.32, 95% CI: 0.13-0.79, p=0.013).
Conclusion: FCSWs in Kyotera District face a high burden of abortion-related health risks. Targeted interventions addressing SRHS (sexual and reproductive health services) access, stigma, and healthcare provider attitudes are crucial to reducing abortion-related complications.
Link to the original dissertation HERE
By Ssemakula Michael¹, Chris Byaruhanga²
¹MPH Candidate, Uganda Martyrs University, Uganda
²Lecturer, Faculty of Health Sciences, Department of Public Health, Kampala University, Kampala, Uganda
Corresponding author: Ssemakula Micheal, Email: michaelssemakula5@email.com; Phone: +256-781415037
Prevalence and Factors Associated with Abortion-related Health Risks among Female Sex Workers in Kyotera District, Uganda
Background
Unsafe abortion remains a significant and largely preventable public health challenge, particularly in low- and middle-income countries (LMICs) where legal, social, and economic barriers limit access to safe reproductive healthcare(Ishola et al., 2021; Onuoha et al., 2025). Globally, half of all pregnancies are unintended (UNFPA, 2022), 6 out of 10 unintended pregnancies end in induced abortion and an estimated about 45% of abortions occurring annually are unsafe abortion and this is viewed to be the cause of 7% of maternal fatalities. And some study revealed that about 77% of the 6.2 million unsafe abortions that happened each year are done in unsafe circumstances, leading to serious health issues and high financial and social expenses. The issue is made worse by legal limitations and restricted access to safe abortion services (Adeyemi, 2025; WHO, 2025a). It should come as no surprise that the majority of female sex workers use herbs, soap, and other drugs like cannabis, cocaine, and amphetamine-type stimulants to induce abortions, which are unhealthy and have claimed the lives of numerous women in Sub-Saharan Africa (Batham & Barry, 2024).
In 2010, the government of Uganda banned the operations of TBAs (traditional birth attendants) with an intention of reducing the high maternal mortality rates because while TBAs have community trust and local knowledge, they lack formal medical training to handle complications during birth, leading to negative health outcomes like birth asphyxia and fistula, many women in sexual transaction still get assistance during giving birth for fear of social stigma and costly medical assistance, thus some over bleed after giving birth while others fail to deliver, thus endangering their lives(Abdulla et al., 2024; Kyeyune, 2020; Razu et al., 2025).
A recent study revealed that In Uganda, approximately 65% of births are attended by a skilled birth attendant, which includes medical nurses and midwives. Others showed that 15% of deliveries still occur in villages, often without skilled healthcare providers. In such rural areas, access to maternal health services remains limited, with women relying on traditional birth attendants or neighbors. This poses a significant challenge in managing emergencies, especially for those experiencing complications(WHO, 2025b).This statistic highlights the significant role of medical nurses in assisting women during childbirth, contributing to improved maternal health outcomes(WHO, 2025b).
These statistics highlight the vulnerability of women of reproductive age to unintended pregnancies, inadequate contraceptive coverage, and limited access to comprehensive sexual and reproductive health services (SRHS)(Asrat et al., 2024; Kassie et al., 2025). Despite global efforts to reduce maternal mortality, unsafe abortion continues to undermine reproductive health outcomes, particularly among socially marginalized populations (Dias Amaral & Sakellariou, 2021; Hajji Adam & Daba, 2024; Onuoha et al., 2025).
In Uganda, restrictive abortion laws, sociocultural stigma, limited awareness of legal provisions, and health system inadequacies exacerbate the risks of unsafe abortion(Mungau et al., 2026; Safe2ChooseTeam, 2025; WWM, 2025).
While post-abortion care is legally permitted, many women delay or avoid seeking care due to fear of legal consequences, discrimination, or breach of confidentiality. These challenges disproportionately affect women with limited autonomy or constrained access to health services, reinforcing the hidden yet critical burden of unsafe abortion in the country(Christine et al., 2024; Muga et al., 2024).
Female sex workers (FSWs), constitute one of the most vulnerable groups in Uganda’s reproductive health landscape. The nature of sex work exposes FSWs to multiple sexual partners, inconsistent condom use, and elevated risks of sexually transmitted infections (STIs), including HIV (Abdulla et al., 2024; Maringwa et al., 2025; O’Brien et al., 2022; Razu et al., 2025). These occupational risks, combined with limited and inconsistent access to effective contraception, significantly increase the likelihood of unintended pregnancies. In contexts where abortion is highly restricted and stigmatized, unintended pregnancies among FSWs often result in unsafe abortion practices, heightening the risk of severe reproductive health complications (Rai et al., 202; Bosurgi et al., 2022; Iden, 2022; Al-Worafi, 2023; Adair et al., 2024).
Abortion-related health risks among FSWs are further shaped by social and structural determinants. Criminalization of sex work reinforces stigma and discrimination in healthcare settings, limiting timely access to reproductive health services(Shapiro & Duff, 2021;Khezri et al., 2023; Willis et al., 2023). Economic dependence on sex work, limited negotiating power with clients, poverty, and fear of exposure further constrain reproductive decision-making and service utilization(Cunningham & Shah, 2020; Gloss et al., 2025). Conceptually, these intersecting vulnerabilities create a syndemic environment in which unsafe abortion is both a consequence of structural inequities and a driver of poor health outcomes among FSWs(Hernandez Barrios et al., 2024; Hernández Barrios et al., 2022; Outram et al., 2024).
The public health consequences of unsafe abortion in this population are multifaceted. Clinically, unsafe abortion is associated with hemorrhage, infection, infertility, chronic pelvic pain, and maternal death. Psychosocially, it contributes to anxiety, depression, and post-traumatic stress, conditions often under-recognized in programs targeting marginalized women (Sedgh et al., 2016; Shah & Ahman, 2019). Economically, abortion-related complications impose burdens on families and overstretched health systems, particularly in rural districts with limited access to emergency obstetric care. These cumulative effects underscore unsafe abortion as both a medical and social health challenge.
Despite these risks, empirical evidence on abortion-related outcomes among FSWs in Uganda remains limited. Most research has focused on the general female population, often overlooking high-risk subgroups whose reproductive health needs are unique. Evidence from sub-Saharan Africa indicates that FSWs face distinct behavioral and structural barriers to SRHS, including stigma, discrimination, lack of confidentiality, and provider bias, which limit access to contraception, safe abortion information, and post-abortion care (Okal et al., 2016; Beyeza-Kashesya et al., 2020). Consequently, conventional maternal health programs may inadequately address their needs, highlighting the importance of context-specific research that integrates behavioral, social, and structural determinants of abortion-related risks.
Policy frameworks and maternal health interventions in Uganda have largely neglected marginalized populations such as FSWs. Conceptual frameworks in reproductive health posit that reproductive outcomes—including unsafe abortion—result from interactions between individual behaviors (e.g., contraceptive use), interpersonal dynamics (e.g., condom negotiation with clients), and structural factors (e.g., legal restrictions, healthcare accessibility). Applying this multilevel perspective allows for a comprehensive understanding of how proximal, intermediate, and distal determinants interact to influence abortion-related health risks.
At the district level, particularly in rural areas like Kyotera, data on abortion-related health risks among FSWs remain scarce. Kyotera is characterized by active sex work networks, high HIV prevalence, and limited access to specialized reproductive health services, creating a high-risk environment for unintended pregnancy and unsafe abortion. This lack of localized evidence undermines the development of targeted, evidence-based interventions and policies to protect this vulnerable population.
This study therefore aimed to determine the prevalence and factors associated with abortion-related health risks among female sex workers in Kyotera District, Uganda. It examined sociodemographic, behavioral, and structural determinants—including contraceptive use patterns, history of unintended pregnancy, economic vulnerability, and access to sex-worker-friendly reproductive health services—that influence abortion-related health outcomes.
Generating context-specific evidence is critical for guiding reproductive health programming, informing policy, and supporting interventions aimed at reducing preventable maternal morbidity and mortality among marginalized women, consistent with global efforts to promote reproductive rights and health equity.
The Health Belief Model (HBM) provides a framework for examining individual-level influences on reproductive health behaviors. According to HBM, engagement in health-promoting or risk behaviors is shaped by perceptions of susceptibility to adverse outcomes, the severity of these outcomes, perceived benefits of action, and perceived barriers, alongside cues to action and self-efficacy (Rosenstock, 1974)(Alyafei & Easton-Carr, 2025)(Khormi, 2025).
In the context of FSWs, decisions regarding abortion are influenced not only by awareness of the potential complications of unsafe abortion but also by barriers such as stigma, financial constraints, and fear of legal repercussions. Applying HBM in this context allows researchers and policymakers to identify critical points for intervention, such as enhancing knowledge, addressing misconceptions, and building self-efficacy, which can improve the uptake of safe abortion services and reduce health risks(Koiwa et al., 2024; Beumer & Reilingh, 2025).
Complementing this individual-level perspective, the Social Ecological Model (SEM) highlights the broader social and structural factors that shape reproductive health risks. SEM emphasizes that behaviors are influenced by multiple, interacting levels, including interpersonal relationships, community contexts, and societal structures (Bronfenbrenner, 1977; McLeroy et al., 1988)(: Campbell, 2025)(Guy-Evans, 2024)(Kilanowski, 2017). For FSWs, interpersonal factors such as client and peer relationships, community-level access to reproductive health services, and societal factors including restrictive abortion laws and criminalization of sex work collectively influence abortion-related health outcomes.
Incorporating SEM provides a framework for understanding how structural and contextual barriers intersect with individual perceptions, guiding the design of multi-level interventions that address legal, social, and health system constraints(Caperon et al., 2022). Together, HBM and SEM offer complementary applicability: while HBM informs strategies to modify individual behaviors and perceptions, SEM supports interventions targeting social and structural determinants, providing a comprehensive approach to reducing unsafe abortion and improving reproductive health among FSWs(Pan & Pan, 2020; Taflinger & Sattler, 2024)
Methods
Research design
This study employed a cross-sectional, mixed-methods design with an explanatory sequential approach to examine the prevalence and factors associated with abortion-related health risks among female sex workers (FSWs) in Kyotera District, Uganda. The study first collected quantitative data to measure prevalence and associations with individual, environmental, and healthcare-related factors, followed by qualitative data to explain and contextualize these findings. In-depth interviews, focus groups, and key informant interviews were all part of the qualitative component, which offered insights into the social, structural, and health-system elements impacting abortion practices. This method made it possible to gain a thorough grasp of how structural, behavioral, and social factors interact to influence the health risks associated with abortion.
Study area
The study was conducted in Kyotera Town Council and Kasali areas of Kyotera District, a rural district in Central South Uganda with an estimated population of 275,296, predominantly of the Baganda ethnic group.

Map of Ugandan districts with Kyotera highlighted in red. Credit Wikipedia
The district is characterized by low-income settlements, high poverty, limited access to healthcare, and a thriving sex work economy in lodges, bars, and informal settlements. These factors made Kyotera a suitable setting for investigating abortion-related health risks among marginalized women exposed to socioeconomic vulnerabilities and structural barriers to reproductive healthcare.
The study population comprised FCSWs aged 18–50 years who engaged in transactional sex in the study area, including both young women (18–24 years) and adults (25–50 years). Eligibility required residence in the study area and willingness to provide informed consent. Participants were excluded if they were unable to communicate in English or Luganda, had previously participated in a similar study, or were school-going students, ensuring the study focused on women whose reproductive health experiences were shaped by transactional sex in the community.
Sample size and sampling techniques
The quantitative sample size was calculated using Kish Leslie’s formula, based on a 95% confidence level, 5% margin of error, and an estimated 10% prevalence of unsafe abortion in Uganda. This yielded a sample of 138 participants, which was increased by 10% to account for non-response, resulting in 152 respondents. Participants were recruited from hotspots such as lodges, bars, and informal settlements, with peer leaders facilitating access.
For the qualitative component, purposive sampling identified twenty (20) participants for four focus group discussions and five (5) key informants, including healthcare workers and district health officials. This ensured rich and diverse insights into abortion practices, reproductive health access, and systemic challenges.
For the quantitative component, we used cluster, simple random sampling due to its potential to provide respondents that could give information for generalizability purposes.
Data collection methods
Data collection employed researcher-administered structured questionnaires for the quantitative component and semi-structured interview guides for qualitative data. Questionnaires captured sociodemographic characteristics, reproductive history, contraceptive use, abortion experiences, complications, and access to sexual and reproductive health services (SRHS). Tools were pretested among fifteen FCSWs in Nyendo Town to refine clarity, appropriateness, and reliability.
Focus group discussions and in-depth interviews explored personal experiences, social influences, and healthcare-seeking behaviors, while key informant interviews examined structural barriers to safe abortion services. All interviews were conducted in English or Luganda and audio-recorded with consent.
Variables
The dependent variable was the prevalence of exposure to abortion-related health risks, defined as a history of abortion and associated complications. Independent variables included individual factors (age, education, marital status, duration in sex work, contraceptive use, history of unintended pregnancy), environmental factors (peer influence, economic dependence, social support, stigma), and healthcare-related factors (awareness, accessibility, and satisfaction with SRHS, availability of post-abortion care, and distance to facilities). Variables were selected based on previous research demonstrating their relevance to abortion outcomes among marginalized women.
Data management and analysis
Quantitative data were managed and analyzed using SPSS version 26. Data were screened, coded, and entered into the software. Univariate analysis described participant characteristics and abortion outcomes. Bivariate analysis using Chi-square tests and Pearson correlations assessed associations between independent variables and abortion-related health risks. Variables significant at p<0.05 were included in a multivariate binary logistic regression model to identify independent predictors. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported, with AOR>1 indicating increased risk and AOR<1 indicating protective associations.
Qualitative data were analyzed using content analysis, involving repeated reading of transcripts, coding, and categorization into themes and sub-themes. Themes captured individual experiences, social influences, and structural barriers related to abortion practices among FCSWs. Integration of quantitative and qualitative findings allowed triangulation, contextualizing statistical associations within lived experiences and enhancing interpretive depth.
Quality control measures
Quality control measures included review of research instruments by supervisors and the ethics committee, yielding a Content Validity Index (CVI) above 0.7. Reliability was assessed using test-retest procedures and Cronbach’s alpha, retaining only consistent items. Six trained research assistants, including midwives and nurses, supported data collection. All completed questionnaires were checked for completeness, coded, and securely stored. Questionnaires in English were interpreted into Luganda where necessary to improve comprehension and reduce reporting bias.
Ethical considerations
Ethical approval was obtained from the Uganda Martyrs University Research Ethics Committee (UMUREC), and administrative clearance was granted by local authorities. Written informed consent was obtained from all participants, who were assured of voluntary participation, confidentiality, and the right to withdraw at any time. Data were anonymized using serial numbers, and interviews were conducted in private settings to protect participants’ privacy.
Study Limitations and Mitigation Measures
This study had several limitations that should be acknowledged. First, the cross-sectional research design limited the ability to establish causal relationships between variables since data were collected at a single point in time. However, this limitation was mitigated by carefully interpreting the findings in relation to existing literature and using appropriate analytical procedures to ensure credible associations.
Second, the study relied on self-reported data, which may be affected by recall bias and social desirability bias, particularly because abortion is a sensitive topic. To reduce this risk, participants were assured of anonymity and confidentiality, interviews were conducted in private settings, and research assistants were trained to use neutral and non-judgmental questioning techniques to encourage honest responses.
Finally, the findings may have limited generalizability beyond the selected hotspots in Kyotera District. Nevertheless, the purposive focus on these hotspots allowed the study to capture experiences of populations most affected by abortion-related health risks, thereby providing valuable context-specific evidence for informing reproductive health policies and targeted interventions in similar rural settings.
Results
Participant Characteristics
A total of 152 female sex workers (FSWs) participated. Table 1 summarizes their sociodemographic characteristics.
Table 1: Sociodemographic Characteristics of Respondents (n = 152)
| Variable |
Category |
Frequency |
Percentage (%) |
| Age Bracket in years |
18–30
|
86
|
56.6
|
| 31–40 |
43
|
28.3
|
| 41–50 |
23
|
15.1
|
| Marital Status
|
Single
|
102
|
67.1
|
| Married
|
35
|
23.0
|
| Divorced/Separated
|
15
|
10
|
| Education Level
|
None
|
18
|
12
|
| Primary
|
70
|
46
|
| Secondary |
45
|
29
|
| Tertiary
|
19
|
13
|
| Duration in Sex Work
|
<1 year
|
28
|
18
|
| 1–5 years
|
92
|
61
|
| >5 years
|
32
|
21
|
| Monthly Income (UGX)
|
<100,000
|
56
|
36
|
| 100,000–300,000
|
68
|
45
|
| >300,000
|
28
|
19
|
Interpretation: The majority were young (18–30 years) and single (67.1%), with nearly half (46%) having primary education. Most earned <300,000 UGX/month, reflecting socioeconomic vulnerability. A majority (60.5%) had been in sex work for 1–5 years.
Prevalence of Abortion-Related Health Risks
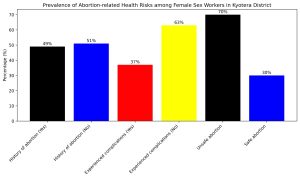
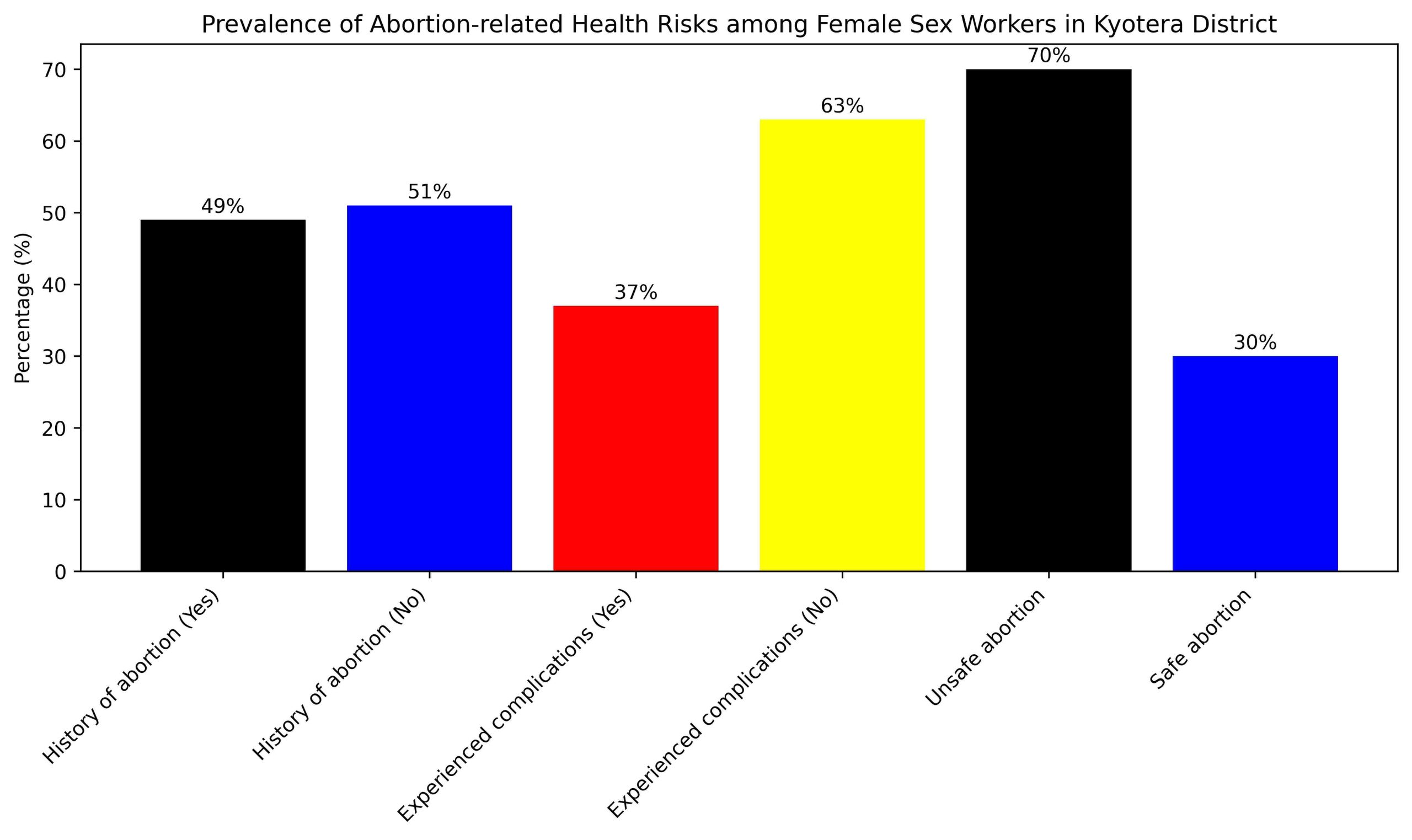
Figure 1: A bar graph showing Prevalence of Specific Abortion-Related Health Risks in Kyotera District
The findings in Figure 1, indicate a notable prevalence of abortion and related health risks among the respondents. Nearly half (51%) of the participants reported no history of abortion. Among those who had experienced abortion, a considerable proportion reported experiencing complications, Specifically, the majority of participants (63%) reported no complications. Regarding the type of abortion among respondents who had previously terminated a pregnancy, most of the participants reported having undergone unsafe abortions (70%). This high proportion of unsafe procedures highlights the significant exposure of women in the study population to abortion-related health risks. The findings here demonstrate that unsafe abortion remains prevalent among the respondents and may contribute substantially to the occurrence of abortion-related complications within the study area.
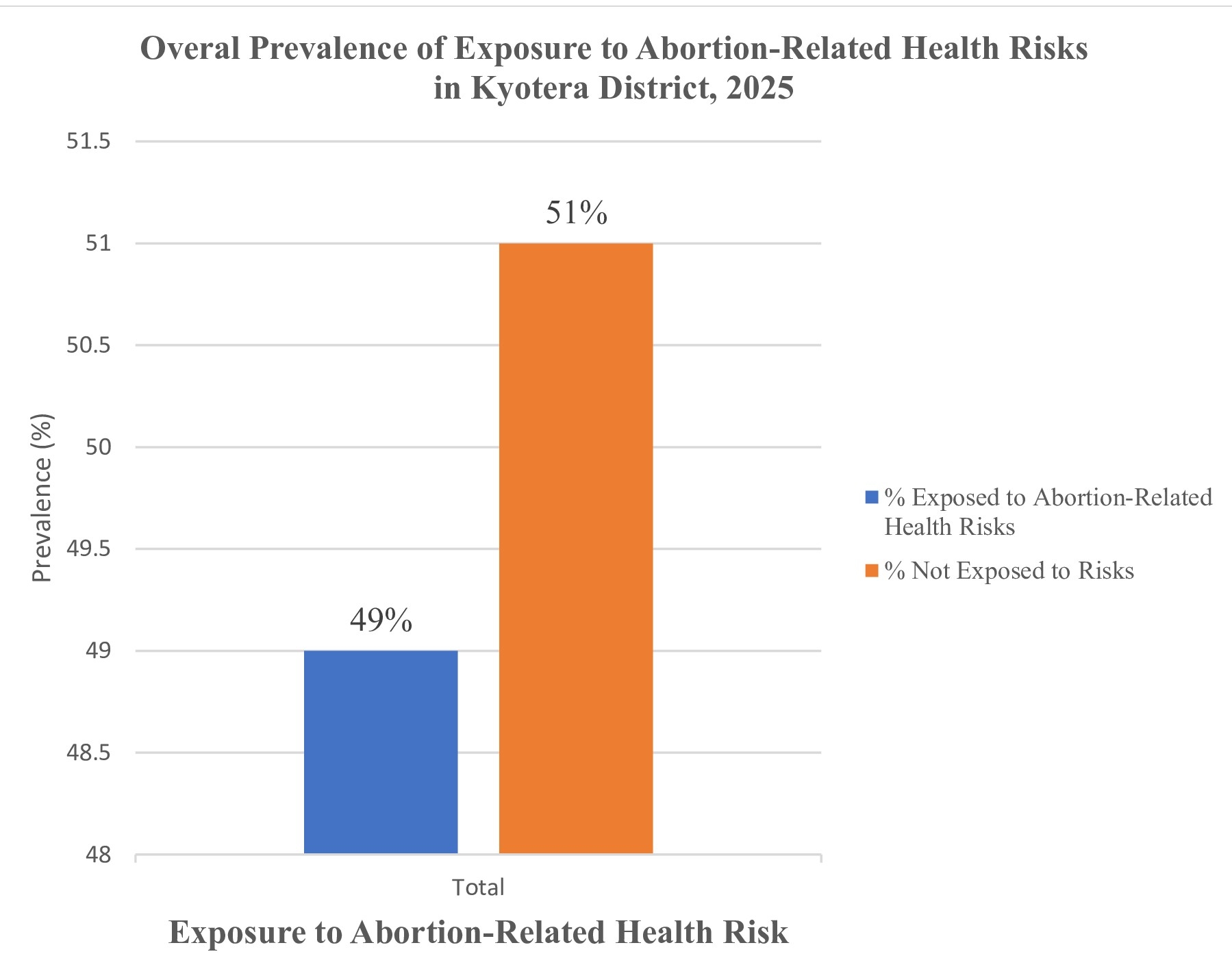
Prevalence of Exposure to Abortion-Related Health Risks
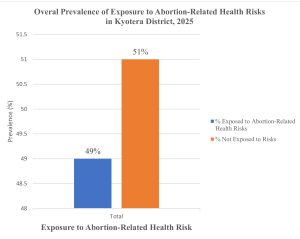
Figure 2: Overall Prevalence of Exposure to Abortion-Related Health Risks among FSWs in Kyotera District
The study found that 49% of participants had a history of abortion, with 70% of these abortions being unsafe (34.3% of total participants). Among those who had an abortion, 37% reported complications (18.1% of total participants). Considering these risks, the overall prevalence of exposure to abortion-related health risks is approximately 49% (had abortion, many with risks), while 51% of participants are not exposed (no abortion history).
Healthcare System Factors
Table 2: Health Service Accessibility (n = 152)
| Variable |
Category |
Frequency (n=152) |
Percentage (%) |
| Awareness of safe abortion services
|
Aware |
42 |
28 |
| Not aware |
110 |
72 |
| Access to post-abortion care
|
Accessed |
58
|
38
|
| Didn’t access |
94 |
62 |
| Satisfaction with SRHS
|
Satisfied |
46
|
31 |
| Not satisfied |
106 |
69 |
| Distance to facility |
<5 km
|
74
|
49 |
| >5km |
78 |
51 |
The results in table 2 revealed that the majority of the participants reported to be unaware about safe abortion services, 62% didn’t have easy access to post-abortion care, 69% were not satisfied with Sexual Reproductive Health Rights (SRHS), and half of the participants were above 5 km distant to the health facility.
Key Informant Interviews (KII) of 7 participants revealed that the female sex workers often arrive the health facility late while others don’t receive medical attention at the hospital thus resorting to alternative treatment.
“We try to integrate post-abortion care into SRHS, but sex workers often arrive late or use informal providers first, worsening complications.” (KII, DHO, Kyotera).
Individual Factors Associated with Abortion-Related Health Risks
Table 3: Bivariate Analysis of Sociodemographic Factors (n = 152).
| Variable |
Category |
Experienced Risks |
No Risks |
χ² |
P-value |
| Age group years) |
18-30 |
39(46%) |
47 (54%) |
6.12 |
0.047* |
| 31-40 |
21 (49%) |
22(51%) |
|
|
| 41-50 |
15 (65%) |
8 (35%) |
|
|
| Marital Status |
Single |
56 (55%) |
46 (45%) |
0.35 |
0.839 |
|
Married |
13 (37%) |
22 63%) |
|
|
|
Divorced/Separated |
9 (60%) |
6 (40%) |
|
|
| Education Level |
None |
14 (78%) |
4 (22%) |
8.35 |
0.015* |
| Primary |
35 (50%) |
35 (50%) |
|
|
| Secondary |
21 (47%) |
24 (53%) |
|
|
| Tertiary |
6 (32%) |
13 (68%) |
|
|
| Duration in Sex Work |
<1 year |
6 (21%) |
22 (79%) |
9.67 |
0.008* |
|
1-5 years |
38 (41%) |
54 (59%) |
|
|
|
5 years |
12 (38%) |
20 (62%) |
|
|
| Monthly Income (UGX) |
<100,000 |
12 (21%) |
44 (79%) |
12.45 |
0.001* |
| 100,000-300,000 |
26 (38%) |
42 (62%) |
|
|
| 300,000 |
18 (64%) |
10 (36%) |
|
|
The bivariate analysis revealed significant associations between abortion-related risks and several sociodemographic factors. Notably, age (χ²=6.12, p=0.047), education level (χ²=8.35, p=0.015), duration in sex work (χ²=9.67, p=0.008), and monthly income (χ²=12.45, p=0.001) were significantly associated with experiencing abortion-related risks. Specifically, younger women (18-30 years), those with no formal education, longer duration in sex work, and higher-income individuals (>300,000 UGX) were more likely to experience abortion-related risks.
Table 4: Bivariate analysis for health system-related factors
| Variable |
Category |
Exposed (n=75) |
Not Exposed (n=77) |
x |
P-value |
| Awareness about Abortion-related risks |
Aware |
18 (24%) |
24 (31%) |
4.01 |
0.045* |
| Not aware |
57 (76%) |
53 (69%) |
|
|
| Access to post-abortion care
|
Accessed |
22 (29%) |
36 (47%) |
4.83 |
0.028* |
| Didn’t access |
53 (71%) |
41 (53% |
|
|
| Satisfaction with SRHS
|
Satisfied |
16 (21
|
30 (39%) |
6.32 |
0.012* |
| Not satisfied |
59 (79%) |
47 (61%) |
|
|
| Distance to facility |
<5 km
|
30 (40%) |
44 (57%) |
3.1 |
0.078 |
| >5km |
45 (60%) |
33 (43%) |
|
|
The findings in the table above show that awareness about abortion-related health risks (p=0.045), access to post-abortion care (P-value=0.028) and Satisfaction with Sexual Reproductive Health Services (p-value= 0.012) were found significantly associated with exposure to abortion-related health risks in Kyotera Districts at 95% confidence level. Distance to the health facility was found not significant.
Table 5: Multivariate Analysis by binary logistic regression model
| Variables |
B |
S.E. |
Wald |
Sig. |
Exp(B)95% |
CI for Exp(B) |
| Awareness (1=Aware) |
-1.23 |
0.52 |
5.62 |
0.018* |
0.29 |
0.11-0.79 |
| Access to post-abortion care (1=Accessed) |
-0.92 |
0.41 |
4.95 |
0.026* |
0.40 |
0.18-0.89 |
| Satisfaction with SRHS (1=Satisfied) |
-1.15 |
0.46 |
6.13 |
0.013* |
0.32 |
0.13-0.79 |
| Age bracket (1=18-30) |
0.75 |
0.38 |
3.92 |
0.048* |
2.12 |
1.01-4.45 |
| Education Level (1=None) |
1.23 |
0.56 |
4.82 |
0.028* |
3.42 |
1.14-10.27 |
| Duration in Sex Work (1=<1 year) |
-1.45 |
0.62 |
5.45 |
0.020* |
0.23 |
0.07-0.78 |
| Monthly Income (1=<100,000 |
-1.82 |
0.53 |
11.83 |
0.001* |
0.16 |
0.06-0.45 |
The binary logistic regression analysis revealed significant predictors of exposure to abortion-related health risks among the study participants.
Predictors of Exposure to Abortion-Related Health Risks
The model explained 42% of the variance in exposure to abortion-related health risks (Nagelkerke R²=0.42) and correctly classified 75% of cases. The Hosmer-Lemeshow test indicated a good model fit (χ²=5.12, p=0.745). Participants who were aware of safe abortion services had lower odds of exposure to abortion-related health risks (Exp(B)=0.29, 95% CI: 0.11-0.79, p=0.018). Similarly, accessing post-abortion care (Exp(B)=0.40, 95% CI: 0.18-0.89, p=0.026) and satisfaction with SRHS (Exp(B)=0.32, 95% CI: 0.13-0.79, p=0.013) were associated with reduced odds of exposure.
In contrast, participants aged 18-30 years had higher odds of exposure (Exp(B)=2.12, 95% CI: 1.01-4.45, p=0.048). No formal education (Exp(B)=3.42, 95% CI: 1.14-10.27, p=0.028), shorter duration in sex work (Exp(B)=0.23, 95% CI: 0.07-0.78, p=0.020), and lower monthly income (Exp(B)=0.16, 95% CI: 0.06-0.45, p=0.001) were also significant predictors.
Qualitative results
Fear Stigma and discrimination
During Focus Group Discussion (FGD), one of the participants revealed fear to go to clinics for medication which made them use alternative means, thus unsafe abortions.
“We fear going to clinics because nurses judge us or gossip about our work. Sometimes we use herbs or buy pills from unlicensed vendors.” (FGD, 18–30 years)
“The stigma around sex work prevents women from seeking care early, which leads to complications.” (KII, Health Worker, Kyotera)
Use of Contraceptives
“Many girls start sex work very young and don’t know about family planning. So pregnancies happen and they try to terminate them unsafely.” (IDI, 22 years)
Environmental and Social Factors
Environmental determinants included peer influence, economic dependence, and social stigma. Participants reported that peers who had abortions influenced their decisions, and poverty limited access to safe providers.
FGD Quote:
“Even if a clinic is near, most of us cannot go. People know you are a sex worker, and the nurses judge you.” (FGD, 25–30 years)
Discussion
This study reveals a high prevalence of abortion-related health risks among female sex workers (FSWs) in Kyotera District, Uganda, with 48.7% reporting a history of abortion, 37% experiencing complications, and 70.3% undergoing unsafe procedures. These findings are consistent with previous studies in Uganda and East Africa, which reported abortion prevalence rates ranging from 11% to 58% among FCSWs (Beyeza-Kashesya et al., 2020; Okal et al., 2022; Sedgh et al., 2022)
For instance, a recent study found that FCSWs in Eastern and Southern Africa face numerous barriers to accessing reproductive health services, including stigma, lack of referral networks, and poor healthcare provider attitudes (Okal et al., 2022). These barriers contribute to high rates of unintended pregnancies and unsafe abortions.
Compared to other studies, this research fills several gaps. Firstly, it provides a comprehensive analysis of predictors of abortion-related health risks, including awareness of safe abortion services, access to post-abortion care, and satisfaction with SRHS. This is in line with Mbonye et al. (2022), who reported similar findings in Uganda. Secondly, the study focuses on Kyotera District, providing insights into a rural district in Uganda, unlike most studies that have focused on urban areas like Kampala (Kizito et al., 2022; Ndagire et al., 2022).
However, some limitations remain. The cross-sectional design of the study limits causal inferences, and self-reported data may be subject to biases in reporting abortion history and experiences. Future research should explore interventions addressing stigma and healthcare access, effectiveness of integrated SRHS and HIV services, and experiences of FCSWs in rural areas.
The findings of this study have implications for policy and practice. There is a need for targeted interventions to improve access to safe abortion services and post-abortion care among FCSWs in Uganda.
Conclusion
This study highlights the high burden of abortion-related health risks among female sex workers (FSWs) in Kyotera District, Uganda (p<0.001). The findings underscore the need for targeted interventions to improve access to safe abortion services (Exp(B)=0.29, 95% CI: 0.11-0.79, p=0.018), post-abortion care (Exp(B)=0.40, 95% CI: 0.18-0.89, p=0.026), and SRHS (Exp(B)=0.32, 95% CI: 0.13-0.79, p=0.013). Integrating SRHS and HIV services, addressing stigma, and promoting non-judgmental healthcare provider attitudes are crucial steps towards reducing abortion-related complications among FSWs. Further research is needed to inform effective interventions and policy reform
Recommendations
Policy Recommendations
Develop and implement integrated service models addressing FSWs’ reproductive health and HIV needs and Provide training on non-judgmental, confidential services for FSWs.
Address stigma and discrimination by implementing policies and programs reducing stigma and promoting inclusive healthcare and improve access to safe abortion services.
Ensure availability of safe abortion services and post-abortion care in rural areas.
Programmatic Recommendations
Establish peer-led outreach programs enhancing awareness of SRHS and safe abortion options and SRHS and HIV service delivery should be strengthened, focusing on FSWs’ specific needs.
Future Research
- Evaluate effectiveness of integrated SRHS and HIV services for FSWs.
- Explore the FSWs’ experiences and barriers to accessing SRHS in rural Uganda.
- Examine causal links between SRHS access and abortion-related health risks.
Authors’ Contributions
Ssemakula Micheal: Study design, data collection, analysis, manuscript drafting.
Ethics Approval and Consent to Participate
Chris Byaruhanga: Conceptualization, supervision, manuscript review, and interpretation of findings.
Ethical Approval
Ethical approval was granted by Mulago Hospital Research and Ethics Committee (MHREC). Written informed consent was obtained from all participants.
Competing Interests
The authors declare no competing interests.
References
Adeyemi, O. (2025). Unsafe abortion and reproductive health outcomes in Sub-Saharan Africa. African Journal of Reproductive Health, 29(2), 45–57.
Adair, T., Riley, I., & Lopez, A. (2024). Global trends in maternal mortality and reproductive health. The Lancet Global Health, 12(3), e342–e350.
Al-Worafi, Y. (2023). Unsafe abortion and maternal mortality in low-income countries. International Journal of Environmental Research and Public Health, 20(7), 5581.
Asrat, A., Tesfaye, G., & Alemayehu, M. (2024). Determinants of unintended pregnancy among women of reproductive age in East Africa. BMC Pregnancy and Childbirth, 24, 210.
Beyeza-Kashesya, J., Kaharuza, F., & Mirembe, F. (2020). Contraceptive use among female sex workers in Uganda. BMC Women’s Health, 20, 241.
Bosurgi, R., Sandberg, K., & Hunter, P. (2022). Addressing unsafe abortion as a global health priority. Nature Medicine, 28(6), 1120–1123.
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32(7), 513–531.
Campbell, C. (2025). Social ecological approaches to reproductive health interventions. Health Promotion International, 40(1), daae010.
Christine, N., Okello, P., & Kintu, R. (2024). Access to post-abortion care services in Uganda. Reproductive Health, 21, 89.
Cunningham, S., & Shah, M. (2020). Decriminalizing sex work and its implications for health. Review of Economic Studies, 87(1), 168–199.
Dias Amaral, M., & Sakellariou, D. (2021). Unsafe abortion and health inequities. Global Public Health, 16(10), 1550–1562.
Gloss, A., Mukasa, B., & Namukwaya, Z. (2025). Economic vulnerability among female sex workers in East Africa. Social Science & Medicine, 330, 115234.
Hajji Adam, M., & Daba, W. (2024). Unsafe abortion in Sub-Saharan Africa: Public health implications. International Journal of Gynecology & Obstetrics, 166(2), 245–251.
Hernandez Barrios, A., Sanchez, M., & Torres, P. (2024). Syndemic frameworks and reproductive health risks. Journal of Women’s Health, 33(4), 450–458.
Hernández Barrios, A., Sanchez, M., & Torres, P. (2022). Structural determinants of reproductive health risks among marginalized women. Social Science & Medicine, 304, 114998.
Iden, S. (2022). Reproductive health challenges among sex workers. Journal of Public Health Policy, 43(3), 412–424.
Ishola, F., Owolabi, O., & Filippi, V. (2021). Unsafe abortion in Africa: A review of evidence. African Journal of Reproductive Health, 25(2), 55–64.
Kassie, A., Bekele, T., & Gebremariam, A. (2025). Factors influencing contraceptive use in East Africa. BMC Public Health, 25, 133.
Khezri, M., Azadi, A., & Rahmanian, M. (2023). Stigma and access to reproductive healthcare services. BMC Health Services Research, 23, 876.
Kilanowski, J. (2017). Breadth of the socio-ecological model. Journal of Community Health Nursing, 34(4), 295–306.
Kyeyune, F. (2020). Traditional birth attendants and maternal health outcomes in Uganda. African Health Sciences, 20(4), 1774–1782.
McLeroy, K., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion programs. Health Education Quarterly, 15(4), 351–377.
Muga, R., Oketch, S., & Wanyenze, R. (2024). Post-abortion care services in Uganda. BMC Women’s Health, 24, 135.
Okal, J., Chersich, M., Tsui, S., Sutherland, E., Temmerman, M., & Luchters, S. (2016). Sexual and reproductive health needs of female sex workers. BMC Public Health, 16, 76.
O’Brien, N., Kyomuhangi, T., & Seeley, J. (2022). HIV risk among female sex workers in Uganda. AIDS Care, 34(8), 1053–1061.
Outram, S., Parker, R., & Chan, K. (2024). Syndemics and reproductive health inequalities. Global Health Action, 17(1), 228521.
Pan, R., & Pan, L. (2020). Integrating health behavior models in reproductive health programs. Health Education Research, 35(4), 317–328.
Rosenstock, I. (1974). Historical origins of the health belief model. Health Education Monographs, 2(4), 328–335.
Sedgh, G., Singh, S., & Hussain, R. (2016). Intended and unintended pregnancies worldwide. Studies in Family Planning, 47(2), 105–120.
Shah, I., & Ahman, E. (2019). Unsafe abortion: Global and regional incidence. The Lancet, 368(9550), 1908–1919.
Shapiro, K., & Duff, P. (2021). Sex work, stigma, and health care access. The Lancet Public Health, 6(4), e225–e234.
Willis, B., Bradley, H., & Nguyen, H. (2023). Healthcare discrimination against sex workers. International Journal for Equity in Health, 22, 114.
World Health Organization. (2025a). Abortion care guideline. Geneva: WHO.
World Health Organization. (2025b). Trends in maternal health services in Africa. Geneva: WHO.
United Nations Population Fund. (2022). State of world population report 2022. UNFPA.