IN A NUTSHELL Editor's NoteThis comprehensive summary provides valuable, evidence-based insights into the hidden oral health crisis in Yemen and offers practical solutions for fragile and conflict-affected settings. It aligns closely with PEAH's mission to address health inequities and advocate for fair access to care for disadvantaged populations
Authors: Mahmood Md. Mohsen Al-Sakkaf¹, Sami A. Hosain Al-Sakkaf²’³, Akram M. Mohammed Al-Sakkaf¹’⁴*, Ahmed A. Abdulrahman Al-Sakkaf²
¹Faculty of Medicine and Health Sciences, Aden University;
²Faculty of Dentistry, Hodeidah University, Yemen
³Center of Tropical Medicine and Epidemiology Studies – Hodeidah University (CTMES-HU)
⁴Special Programme for Research and Training in Tropical Diseases (TDR)
Type of Manuscript: Review Article / Textbook Synopsis
Note: This manuscript describes the content, structure, and evidence base of a forthcoming textbook on oral public health and epidemiology in Yemen. The full textbook is approximately 85,000 words with 20 chapters.
*Corresponding Author:
Dr. Akram M. Mohammed Al-Sakkaf, MBChB, MPH
Email: Akram.m.alsakkaf@gmail.com
Oral Public Health and Epidemiology: Foundations for Action in Yemen – A Textbook for Students and Researchers in Fragile and Conflict-Affected Settings
ABSTRACT
Background: Yemen has experienced a protracted armed conflict since 2015, facing one of the most severe humanitarian crises in recent times. The ongoing conflict has forced over 4 million people from their homes and devastated nearly half of the country’s healthcare facilities, and more than 80% of the population living in poverty. About 79.3% of adults are suffering from periodontitis, and between 50% and 60% of long-term Qat chewers have potentially malignant oral lesions and most of dental caries remain untreated. Moreover, Yemen lacks a national oral health survey or an oral cancer registry, and no fluoridation programme at the population level. Additionally, the dentists-to-population ratio is less than one dentist for every 50,000 people; far below the WHO’s recommendation of one for every 5,000
Objectives: This textbook aims to address these issues by offering a detailed guide to oral public health and epidemiology tailored specifically for Yemen. It takes global frameworks and adjusts them to fit the unique challenges of conflict-affected settings, pulling together all the peer-reviewed research available from Yemen.
Target Audience: undergraduate and postgraduate students studying dentistry, medicine, nursing, and public health; researchers working in fragile environments; and clinicians, policymakers, and humanitarian workers who are either in Yemen or places facing similar challenges.
Structure and Content: The textbook is organized into four parts with 20 chapters and six appendices. The first part covers the core concepts and social determinants of health. The second part focuses on periodontal diseases, caries, oral cancer, and local risk factors. Part three provides guidance on conducting research in conflict zones. Part four part covers health promotion strategies, prevention methods, rebuilding health systems post-conflict. In addition, dedicated chapters on Qat harm reduction, traditional tobacco use, malnutrition concerns, and fluorosis. Practical resources include consent forms available in both Arabic and English.
Conclusion: This textbook fills a crucial gap by providing an evidence-based resource tailored for oral public health in Yemen. It stands as an essential reference not just for students and researchers but also for clinicians and policymakers not only in Yemen but also in other fragile settings around the world.
Keywords: Qat chewing; periodontitis; dental caries; oral cancer; Shammah; Al-Tambal; fluorosis; conflict setting; fragile state; internally displaced persons; task‑shifting; universal health coverage; harm reduction; prevention and health promotion; social determinants of health.
INTRODUCTION
Yemen has been in a protracted armed conflict since 2015, and it has resulted in one of the most severe humanitarian crises faced in this century. According to a 2023 report from the United Nations Development Programme (UNDP), over 4 million individuals have been forced to flee their homes, and nearly half of the health facilities are either barely functioning or completely destroyed. On top of that, over 80% of the population lives below the poverty line [1].
Oral diseases are quietly spreading like a hidden epidemic. A recent study conducted in Sana’a in 2026 found that 79.3% of adults are suffering from periodontitis [2]. Other research indicates that around 50-60% of long-term Qat chewers end up developing potentially malignant oral lesions [3-5]. Dental caries is largely untreated, particularly in children and according to the Global Burden of Disease (GBD) study, approximately 3.7 billion people globally are suffering from dental caries and untreated dental caries is actually the most common health problem [6].
The situation is exacerbated by Yemen’s fragile health system; no national oral health survey since 1990, there is no registry for oral cancer, and no programmes for water or salt fluoridation. In rural areas, the dentists-to-population ratio is concerning; there is often less than one dentist for every 50,000 residents. Low-income countries typically have around 0.55 dentists for every 10,000 people, which breaks down to about one dentist for every 18,000 persons. The World Health Organization (WHO) actually recommends having a dentist for every 5,000 people [7-9]. This shortage really hits hard in these rural communities [7], makes it so much harder for people to get the dental care they really need.
When the authors went looking for a textbook on oral public health and epidemiology that fits Yemen’s unique challenges, they found a significant gap. Most international textbooks operate under the assumption that there is stable governance and some basic infrastructure conditions that definitely do not apply to Yemen right now. They lack advice on how to carry out an oral health survey in a displacement camp or how to adapt WHO criteria when you do not even have a dental chair available. This textbook aims to bridge this gap and is designed as a comprehensive guide on oral public health and epidemiology specifically for Yemen. It takes those global frameworks and adapts them to fit the unique challenges that come with being in a conflict zone. Furthermore, it brings together all the important peer-reviewed research that are available from Yemen, making it highly relevant for anyone interested in this field.
METHODS-BOOK STRUCTURE
The textbook is divided into four main parts with a total of 20 chapters and six appendices. It is designed with a solid foundation in public health education while also being tailored to fit the unique context of Yemen. Figure 1 shows how the textbook is structured into four connected parts. It starts with the foundations in Part One, then moves through epidemiology and risk factors in Part Two. Next up is Part Three, which dives into research methods, and it all wraps up with public health action in Part Four. This framework is backed by three core public health functions: assessment, policy development, and assurance [10] taking into account the specific challenges faced in Yemen, including conflict, Qat use, tobacco issues, malnutrition, and fluorosis. This framework is inspired by the Dahlgren-Whitehead rainbow model [11] adjusted to address the unique challenges faced by areas like Yemen, where conflict and instability are part of everyday life.
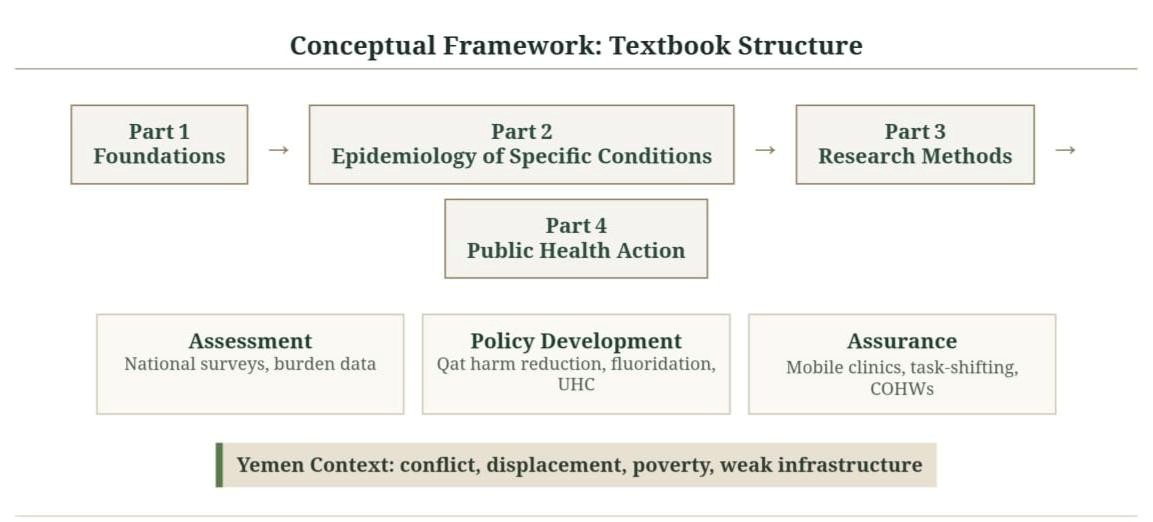
Figure 1: Conceptual Framework of the Textbook Structure. Four integrated parts flow from foundations to public health action, supported by the three core functions of public health and the Yemen‑specific context
- Part One: Foundations of Oral Public Health (Chapters 1-4) – Figure 2 (Conceptual Framework)
This part sets the stage for understanding oral public health, especially in vulnerable settings. In Chapter 1, begin by breaking down what oral public health actually is and how it stands apart from clinical dentistry. The three core functions of public health: assessment, policy development, and assurance were defined by the Institute of Medicine’s insights from way back in (1988) [10]. Chapter 2, looks at the global burden of oral diseases, throwing in some eye-opening stats from Yemen, heavily leaning on findings from the GBD Study [6]. Chapter 3, discusses how conflict, displacement, poverty, and Qat culture impact on oral health issues in Yemen using the Dahlgren-Whitehead rainbow model [11] to help illustrate these connections. Chapter 4 wraps up with some essential epidemiologic principles like prevalence and incidence and using real data from Yemen to bring those concepts to life [12,13].
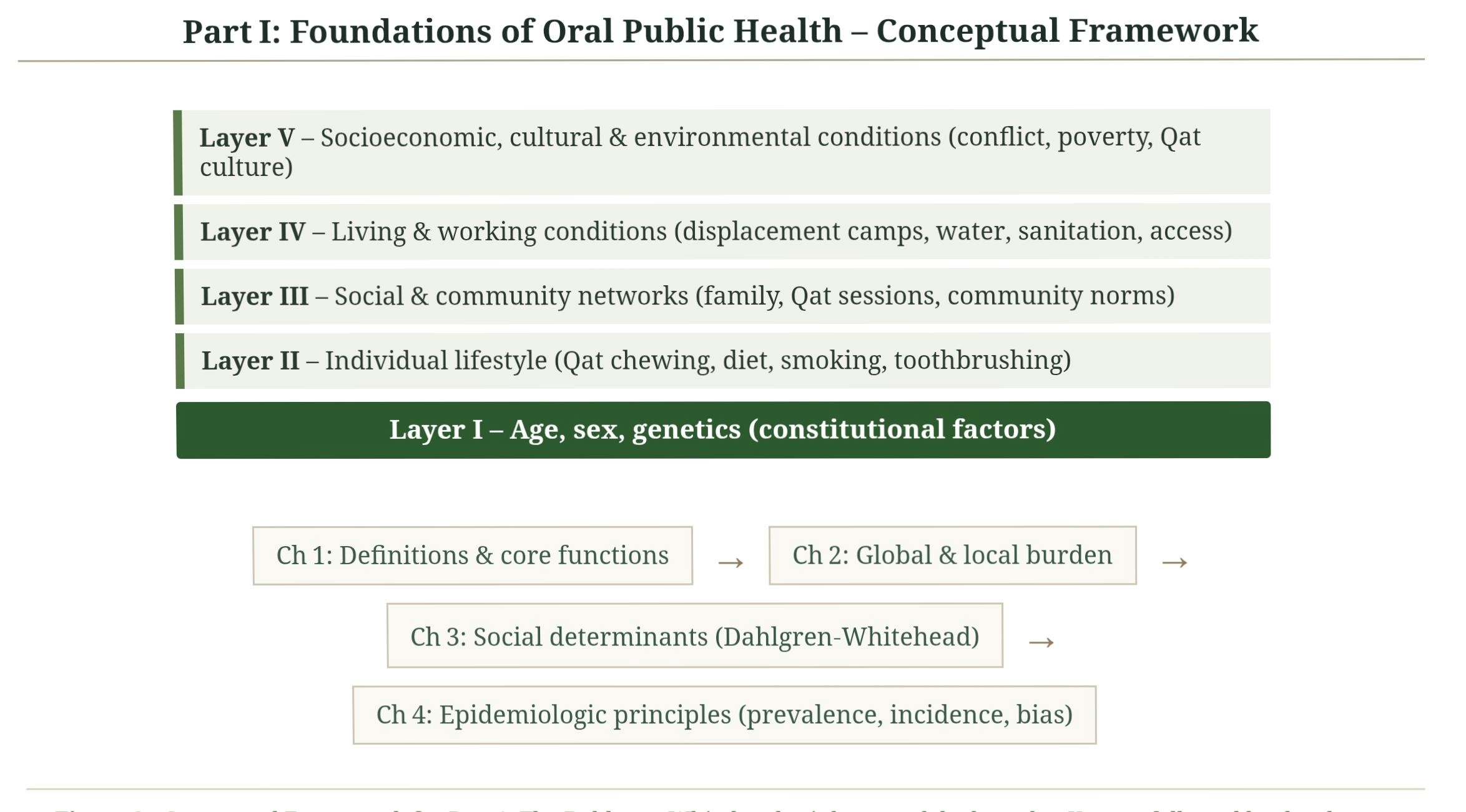
Figure 2: Part One Conceptual Framework. Foundations of Oral Public Health. Four Chapters follow from core definitions to epidemiologic methods. Adapting the Dahlgren-Whitehead rainbow model to Yemeni context
- Part Two: Epidemiology of Specific Conditions (Chapters 5-10) – Figure 3 (Conceptual Framework)
In this part, applies epidemiologic concepts and methods and diving into some specific oral diseases that are particularly relevant to Yemen. Chapter 5 zooms in on periodontal diseases, drawing on insights found from recent Sana’a study [2] and current classification systems [14]. Chapter 6, addresses dental caries, from the sugar-fluoride balance to the tricky issue of getting access to restorative care [6,14-18]. Chapter 7 focuses on oral cancer and potentially malignant lesions using evidence from local studies [3,4,19,20] and research from around the world [21-23]. Chapter 8 takes a look at developmental and genetic oral conditions while shining a light on consanguineous marriage a practice that is common in about 40-60% of Yemeni marriages [24]. Chapter 9 discusses some unique risk factors in Yemen including Qat use [25], Mada’a waterpipe [25,27], smokeless tobacco products i.e., Shammah [5,28] and Al-Tambal (betel quid) [21] along with burning issues like malnutrition and vitamin D deficiency [29] and endemic fluorosis [30]. Chapter 10 looks into oral health among special populations including children, the elderly, and those who have been internally displaced [31,32].
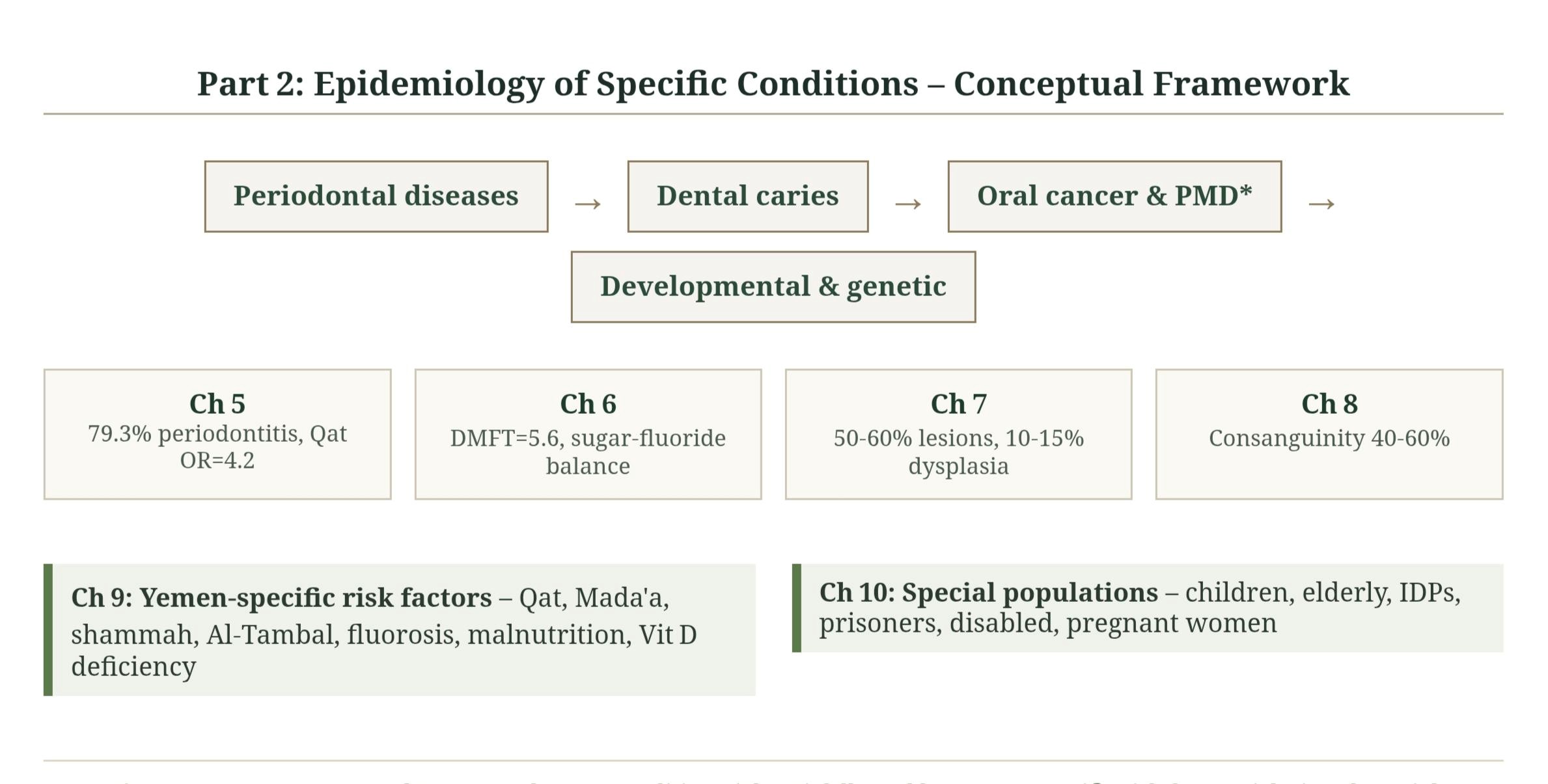
Figure 3: Part Two Conceptual Framework. Epidemiology of Specific Oral Public Health Conditions. Ch 5-8 Core conditions, followed by Yemen‑specific risk factors (Ch 9) and special populations (Ch 10). *PMD = Potentially Malignant Disorders
- Part Three: Research Methods in Oral Epidemiology (Chapters 11-16) – Figure 4 (Conceptual Framework)
This part dives into practical tools for conducting oral health research in fragile and conflict zones. Chapter 11 discusses various study designs that fit the situation in Yemen [33,13]. Chapter 12 addresses sampling methods and survey techniques, drawing from Levy & Lemeshow and the WHO [34,9]. Chapter 13, a thorough discussion of measurement based on WHO guidelines, including how to calculate and understand the kappa statistic thanks to Landis & Koch and the WHO again [34,9]. Moving on to Chapter 14, data management and analysis, along with some software options discussed, with insights from the CDC and R Core Team [35,36]. Chapter 15 discusses challenges may be faced by researchers in conflict areas from getting ethical approvals when review boards are non-functional to figuring out informed consent for individuals with low literacy citing Ford et al. and the WHO [37, 38]. Chapter 16 zooms in on ethical issues specific to oral health research in fragile states, referencing both the Belmont Report and the Declaration of Helsinki [39,40].
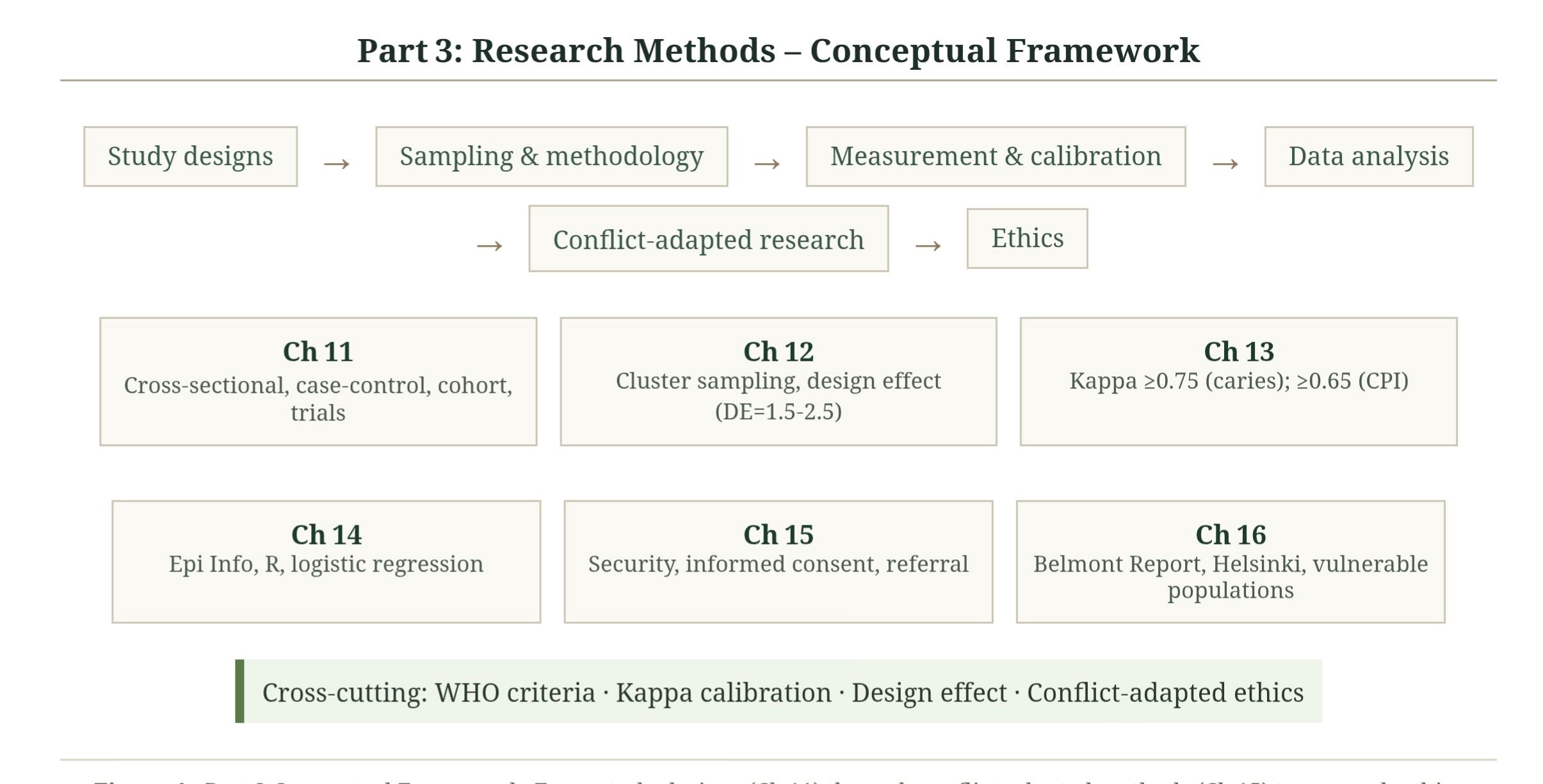
Figure 4: Part Three Conceptual Framework. Research Methods in Oral Epidemiology from study designs (Ch 11) through conflict‑adapted methods (Ch 15) to research ethics (Ch ’6)
- Part Four: Public Health Action (Chapters 17-20) – Figure 5 (Conceptual Framework)
This part focuses on how we can take what we have learned from epidemiological studies and put it into action for public health. Chapter 17, dive into health promotion and education strategies, integrating behavior change theories such as the Health Belief Model from Becker [41] Social Cognitive Theory by Bandura [42]. In addition, Ottawa Charter for Health Promotion and the Transtheoretical Model [43,44]. Chapter 18 explores evidence-based prevention strategies. Discussions about fluoride interventions [45,46] and sugar reduction initiatives [18] not to mention Qat harm reduction and school-based programmes. Chapter 19, discusses how health systems can better support oral health in Yemen. This includes integrating oral health into primary care and other methods aimed at reaching universal health coverage [46,47]. Finally, in Chapter 20, presents a vision for rebuilding oral health in a peaceful Yemen; drawing inspiration from lessons learned in other post-conflict countries [48,49,50] and the WHO Global Oral Health Action Plan [51].
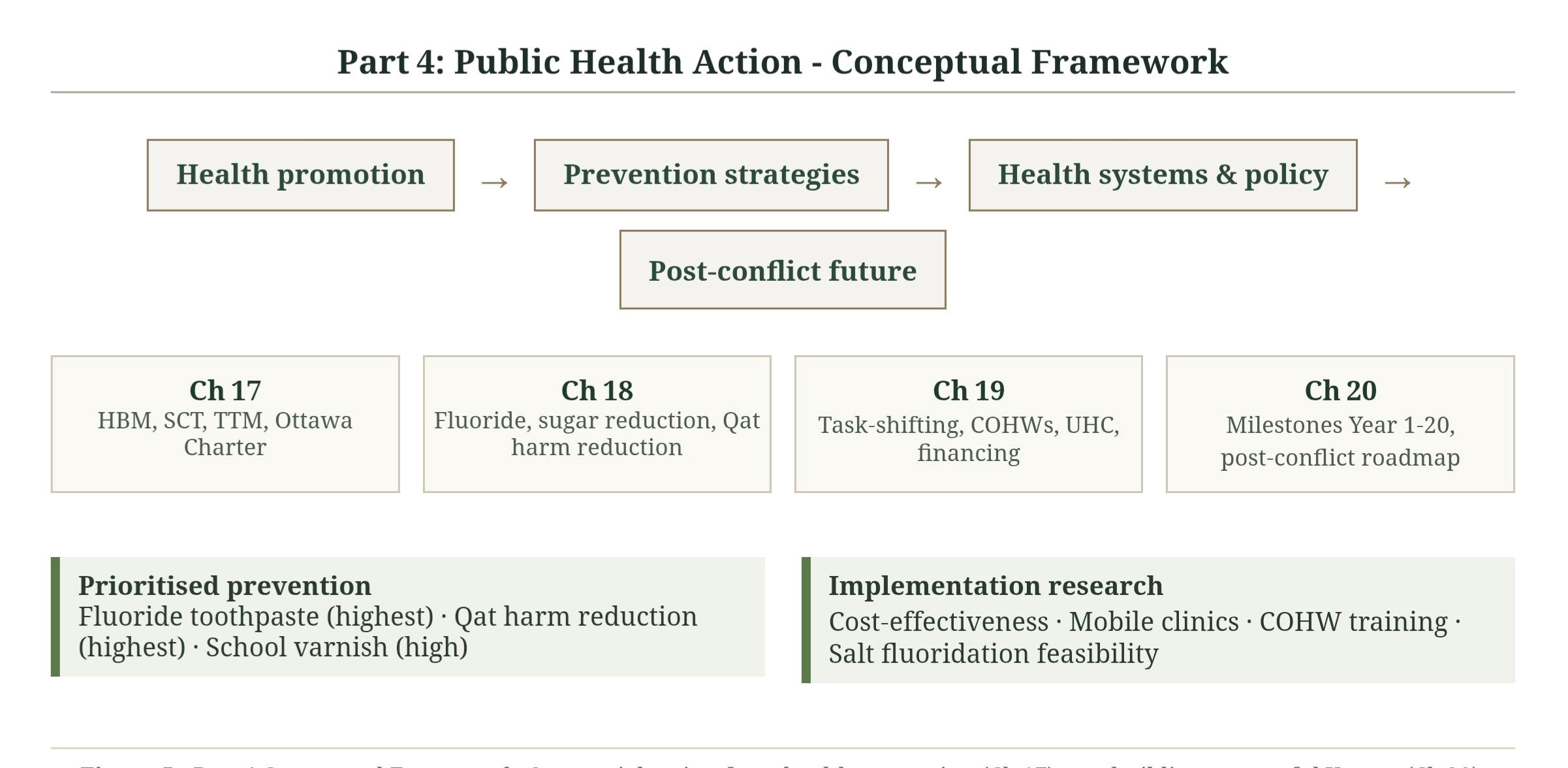
Figure 5: Part Four Conceptual Framework. Public Health Sequential Action from health promotion (Ch 17) to rebuilding a peaceful Yemen (Ch 20)
- Appendices
Six appendices were provided include practical tools such as an adapted WHO-based oral health assessment form for field use in Yemen; sample consent forms in both Arabic and English; an examiner calibration protocol; statistical tables; a sample dataset for student activities; plus a detailed glossary. There’s also back matter with answers to review questions and an index that’s fully cross-referenced for easy navigation.
RESULTS / KEY FINDINGS FROM THE YEMENI EVIDENCE BASE
Some key epidemiological findings from Yemen integrated throughout the textbook which help grasp the burden, distribution, and risk factors of oral diseases in conflict and fragile state.
- Periodontal Disease Burden and Risk Factors
A recent cross-sectional study in Sana’a by Alhajj and colleagues in 2026 [2] assessed the oral health of 450 adults between 18 and 65 years old, using the WHO Community Periodontal Index (CPI) and found that around 79.3% of urban Yemeni adults were found to have periodontitis, with almost a third at severe stage-pocket depths of ≥6 mm, ranking Yemen among the countries with the highest periodontal disease prevalence globally. This is not just about genetics or luck: several behavioral risk factors were identified i.e., 68.8% of men and 12.7% of women reported daily or near daily Qat chewing. Smoking was also prevalent, with 24.2% of participants were current smokers and only about 22.2% brushed their teeth twice a day. When they further analyzed the numbers using multivariable logistic regression, five main risk factors emerged for periodontitis. Daily Qat chewing was the strongest (adjusted OR = 4.2; 95% CI: 2.8-6.3; p < 0.001), followed by being over 45 years old (OR = 3.5; 95% CI: 2.2-5.6; p < 0.001), having diabetes mellitus (OR = 2.8; 95% CI: 1.6-4.9; p = 0.003), brushing teeth less than once a day (OR = 2.3; 95% CI: 1.5-3.6; p = 0.001), and current smoking (OR = 2.1; 95% CI: 1.4-3.2; p = 0.002) [2].
When it comes to prevention, these findings are significant for public health. Basically, when calculating the population attributable fraction (PAF) in order to understand how many cases of periodontitis could be prevented if everyone just stopped chewing Qat. Using the formula PAF = Pe(OR-1)/[Pe(OR-1)+1] where Pe = 0.402 is the rate of daily Qat chewing at around 40.2%, the PAF = 56.3%; meaning that more than half of periodontitis cases (56.3%) could be potentially prevented. This shows how important it is to focus on harm reduction strategies for Qat use; a clear call for action.
- Qat-Associated Oral Lesions and Their Malignant Potential
In this regard, the textbook synthesises multiple studies that explore oral lesions linked to Qat chewing in Yemen, helping readers grasp just how serious this habit can be.
Al-Sharabi and colleagues in 2013 conducted a landmark study comparing 500 Qat chewers to non-chewers in Sana’a and found that white lesions appeared at the chewing site for about 58% of Qat chewers compared to just 4% among non-chewers; biopsy revealed that while most were benign hyperkeratosis, about 12% showed dysplastic changes which may progress to cancer [3]. Another study among long-term Qat chewers confirmed a dose‑response relationship the longer duration of Qat chewing, the higher their risk becomes for serious health issues and malignant potential [4].
A systematic review by Hassan and colleagues took a broader look at six studies from both Yemen and Somalia and reported that around half 52% (95% CI: 44‑60%) of Qat chewers had oral lesions, with dysplasia appearing in about one out of every nine lesions analyzed 11% (95% CI: 6‑16%) [19].
A histopathologic study by Ali examined biopsies from chronic Qat users and comparing tissues from both sides of their mouths “chewing vs non-chewing” and demonstrated marked localised damage caused by Qat use: thickened layers (acanthosis) on the chewing side were seen in nearly all samples 88% versus 0% on the non‑chewing side. Notably when combined with smoking, risks skyrocketed with epithelial dysplasia was present in about 41% of smokers who also chewed Qat compared to 9% among those who did not smoke at all [20]. This insight is pivotal for clinical practice and is emphasized throughout the textbook.
- Shammah: A Group 1 Carcinogen in Widespread Use
Next up is Shammah a powdered smokeless tobacco product classified as a Group 1 carcinogen by the International Agency for Research on Cancer (IARC) [22]; which means there is a solid evidence that is causes cancer in humans (carcinogenicity).
In a recent systematic review (2025) by Museedi and colleagues, synthesising 40 studies from the Middle East and reported some alarming findings that using Shammah was associated with an odds ratio of 3.9 (95% CI 2.5-6.2) when it comes to the risk of oral cancer, which definitely indicates a significant increase in risk. On the other hand, Qat chewing had a pooled odds ratio of 2.7 (95% CI 1.9-3.8) pointing out that it is risky too, just not to the same extent as Shammah [5].
A study by Scheifele and colleagues involving 200 Shammah users across Yemen revealed that 31% had mucosal burns, primarily located on the tongue or floor of the mouth – high‑risk sites for oral cancer. They also found oral leukoplakia present in about a quarter of users along with two documented cases of oral squamous cell carcinoma [28]. What is really alarming is that only about one-fifth (19%) of Shammah users knew it could cause cancer; a major gap in public health education addressed later on in the textbook’s health promotion sections [28].
Factors like age, non-formal or primary education, previous Shammah use, and frequency of use per day were played significant roles too and independently associated with the presence of such lesions [28]. The textbook helps readers make sense of these relationships by discussing dose-response relationships to illustrate risk gradients like how using Shammah for more than five minutes significantly raises risk level compared to shorter use times.
On a more positive note, several protective factors emerged too. Rinsing after applying Shammah seemed to lower risk substantially while knowing its carcinogenicity made a difference too showing potential pathways for harm reduction strategies moving forward [28]
- The Dual Burden of Fluoride: Fluorosis and Caries
The textbook also examines the paradoxical fluoride situation in Yemen. The fluoride levels found in groundwater across various regions far exceed what is deemed safe by WHO 1.5 mg/L where in some areas i.e., Sana’a, Taiz, Ad Dhale’e, Ibb, and Dhamar hit the levels “reaching up to thirty-two mg/L” [9]. In a large survey involving over seventeen thousand schoolchildren conducted by Al-Akwa and colleagues found that around two-thirds of children had dental caries [30]. Beyond the general paediatric population, orphaned children face additional challenges when it comes to their dental health, and it is often tougher for them than for other children. A study from 2025 looked at 644 orphans aged 6 to 10 in Ibb and Al-Hodeidah and found that around 7.8% had already lost their early primary molars. It is pretty eye-opening to see how the region impacts their dental issues, showing just how vulnerable these children truly are [18].
An inverse relationship (negative correlation) was observed between fluoride levels and caries experience with the lowest caries scores at the optimum fluoride level of 0.61‑2 ppm while the highest scores at the two extremes (0.0‑0.4 ppm and >2 ppm), demonstrating the characteristic U‑shaped relationship between fluoride exposure and dental caries [30]. To break down fluoride toxicity, the textbook outlines how fluorosis progresses as exposure increases from mild mottling at lower levels to severe deformities as concentrations climb higher than ten mg/L [9].
- Workforce and Access to Care
The textbook addresses workforce issues within Yemen’s oral health sector which are quite pressing right now. A recent study highlighted gaps among general dental practitioners regarding techniques such as stainless steel crowns and Hall technique, findings that over eighty percent of dentists felt they needed additional training [52]. Younger dentists under thirty seemed more open to using advanced methods which hints at shifts happening within clinical practices over time but quite a few learned these techniques informally through platforms like YouTube rather than through formal education systems. The disparities observed between northern/middle versus southern regions regarding technology usage (p < 0.001), reflecting the fragmented nature of health services in Yemen [52]. These findings guide discussions around important strategies like task-shifting or mobile clinics as ways to tackle workforce shortages effectively across Yemen’s health landscape.
DISCUSSION
This textbook represents a significant advance; being the first to address oral public health and epidemiology in Yemen. It brings together what’s known about the situation in Yemen, points out some significant gaps in research, and provides practical solutions for dealing with health issues in conflict zones.
Some of the findings from the current available studies are downright shocking: such as, 79.3% of people have periodontitis associated with Qat chewing, nearly half to 60% of those who chew it long-term end up with oral lesions, and around 10-15% showing signs of dysplasia, and the significant high odds ratio for developing oral leukoplakia among Shammah users OR=12.99. More than two-thirds of school children in highland areas are battling endemic fluorosis. These numbers really bring home just how serious the oral health crisis is in Yemen and show how urgent it is to take action. Oral health problems in Yemen are pretty similar to what we have seen in other conflict-affected areas in the Middle East. For instance, a study from Gaza in 2025, showed that nearly 30% of dental patients had oral lesions, and more than 19% were found to have potentially malignant disorders. It just goes to show how widespread these oral health challenges are among populations living through the chaos of war in the region [53].
Contribution of the Textbook
This textbook breaks new ground in the field of oral public health, especially when it comes to fragile and conflict-affected places like Yemen.
For starters, it is the first comprehensive guide tailored specifically for Yemen. Many international textbooks just assume there is stable governance and functioning health services, which is far from the reality in Yemen right now. This textbook adapts the current well-established international frameworks i.e,. the WHO Oral Health Survey Manual [9] to fit the context-specific challenges faced by a country in crisis. As Dahlgren and Whitehead pointed out, effective public health needs to tackle multiple layers of factors, and this textbook does just that, ranging from individual behavior change to advocating for national policies [11].
It also dives deep into specific risk factors that are particularly relevant to Yemen but often missed from standard literature. For instance, it discusses the traditional Mada’a waterpipe, which can deliver nicotine equivalent to approximately 70 cigarettes in a single session [25]. And when people mix that with Qat chewing, it significantly increases the chances of developing epithelial dysplasia [5,28]. The book does not shy away from smokeless tobacco products like Shammah either, which have been linked to a high risk of oral lesions [5,19,28]. Furthermore, it highlights the odd situation where both endemic dental and skeletal fluorosis alongside rampant dental caries in different areas definitely a phenomenon rarely addressed in standard health textbooks.
Moreover, this textbook provides practical guidance on conducting research in conflict zones, which is pretty hard to come by elsewhere. It lays out protocols for getting ethical approval even when institutional review boards are non-functional [37], safety planning for research teams, and how to get informed consent from individuals with limited literacy levels. It also suggests ways to create referral pathways for participants needing treatment and how to share findings with various audiences effectively. As the WHO has pointed out, doing research in fragile settings requires some substantial adaptations that are not covered in standard research guides [38].
Given that Yemen has fewer than one dentist per 50,000 people in rural areas [7,8,9], this textbook dives into some practical solutions, like task-shifting and training up community oral health workers, these strategies are important for getting care to more peoples. The authors take inspiration from successful models in other low-income countries and adapt them to fit Yemen’s specific needs.
Target Audience and Utility
This textbook is designed for a diverse audience. Undergrads studying dentistry, medicine, nursing, or public health will find foundational concepts paired with Yemeni case studies and review questions. Postgraduate researchers can dig into advanced methods and gaps in research with detailed answer keys provided. Clinicians and general practitioners will benefit from the emphasis on social determinants of health and hands-on strategies such as dealing with Qat-related lesions and reduction strategies which can be directly applied in their daily practice. Plus, health policymakers and humanitarian workers will find solid guidance on strengthening health systems, financing strategies, task-shifting approaches, universal health coverage principles, and even tips on ethical resource allocation.
Further, the authors rely on legitimate peer-reviewed studies and acknowledging the gaps either if there is no enough Yemeni data, like national surveys or cancer registries, they highlight those areas where more research is desperately needed.
Limitations
There are a few key limitations to keep in mind when looking at the scope and generalizability of this textbook and how applicable it really is.
First, the information we have on oral health in Yemen is pretty limited. It has been ages (since 1990, to be precise) since there has been a national survey on oral health. Second, no national oral cancer registry-limited data on the actual numbers to accurate understanding of the oral cancer situation in Yemen. Third, when it is comes to traditional Yemeni habits and risky behaviors like the Mada’a waterpipe, Shammah, and Al-Tambal (betel quid), little epidemiological research has been done. No prospective longitudinal studies to track how these products impact health over time and no randomized controlled trials to see if any harm reduction methods actually work. Fourth, the textbook suggests some solid solutions for improving the health system, like adding fluoride to salt, taxing sugary stuff, and shifting-tasks among healthcare workers. But here is the thing: these suggestions depend on a level of governance and stability that is not happening in Yemen right now. Thus, putting these ideas into action will not be straightforward and need to take it step by step, starting with some pilot programmes, and of course significant international support will be crucial to make any real progress. Fifth, the textbook can definitely might have its own biases, especially when it comes to publication and geography. Sixth, the practical advice in the textbook for doing research in conflict zones has not really been officially validated. A lot of the adjustments made to the WHO methods like using fewer sampling clusters, trading dental lights for headlamps, and simplifying consent forms are based more on what the authors have seen in the field and what experts suggest rather than solid proof. Also, while the focus is on Yemen, those adjustments might not necessarily fit well in other unstable regions without a bit of extra customization to fit local culture, politics, and health concerns. However, as mentioned earlier, the oral health problems in Yemen could really be a snapshot of what’s happening in other conflict-affected areas throughout the Middle East [53].
Finally, it is clear that even though the authors tried to stay objective, their own opinions and priorities definitely peek through in the textbook. They really focus on oral health and public health research, and that shapes what gets included. However, other stakeholders perspectives like Qat farmers, traditional tobacco users, patients fighting oral cancer, or even humanitarian aid workers was not systematically explored during the writing process. Bringing in those different perspectives would make future editions much better.
Implications for Policy and Practice
Even with these limitations, the textbook suggests a few important points for oral health policy in Yemen.
Prevention: We really need to step up Population-wide fluoride programmes urgently. Pushing for salt fluoridation sounds like a solid long-term plan, but right now, getting fluoride varnish into schools should be of top priority. Qat harm reduction, when we talk about qat use, let’s focus on promoting safer practices like chewing on different sides, rinsing, doing self-checks, and making sure people get screened annually without condemning anyone for their choices. For people’s in areas with high fluoride levels (Taiz, Ibb, Dhamar, and Ad Dhale’e), finding alternative water sources and setting up home filtration systems is crucial to tackle fluorosis issues.
On the workforce side: shifting some tasks to COHWs (who just basic training) and Dental Nurses (who train for two years) is highly important. If we aim for one COHW for every 10,000 people, we are looking at needing around 3,000 of them across the country. That’s totally achievable within five years if we can get some international support.
Health system: It is essential to create a national oral health policy that dedicates at least 1% of the health budget to this area. Oral health must be integrated into primary care and Universal Health Coverage. Furthermore, basic services package that covers education, fluoride varnish application, atraumatic restorative treatment (ART), extractions, and dentures would cost around $2-3 per person each year.
As for research priorities include national surveys, set up an oral cancer registry, collect pediatric data, conduct economic analyses, and run longitudinal studies on traditional risk factors. Plus, intervention trials will play a key role in shaping our national research agenda. Partnerships with international organizations are essential for boosting our research capacity as well.
CONCLUSION
“Oral Public Health and Epidemiology: Foundations for Action in Yemen” addresses a significant gap in the available literature. It is a comprehensive, evidence-based guide designed for oral public health education and professionals in Yemen, tailoring global public health concepts to meet the distinct challenges that arise in a country affected by conflict and in fragile states. The textbook synthesises a wealth of peer-reviewed studies from Yemen. For instance, some recent research shows that approximately 79.3% of people have periodontitis, which is strongly linked to Qat chewing [2]. Additionally, there are alarming rates of oral lesions linked to Qat use, 50-60% of users are affected, with 10-15% showing dysplasia [3,4]. Shammah users have an odds ratio of 12.99 for developing leukoplakia, whereas only 19% know it can lead to cancer [5,28]. Finally, the widespread issue of fluorosis among schoolchildren, where dental caries has a prevalence rate of 67.6% [30].
In summary, this textbook extends beyond data; it offers practical advice that has been tested in the field. There are strategies for research in conflict zones, models for task-shifting, designs for mobile dental clinics, and culturally sensitive ways to reduce harm from Qat. It is set up for open-access publication, making it a reference for dental and public health students, researchers, clinicians, and policymakers not just in Yemen but also in other fragile areas around the globe. The authors welcome feedback and contributions for future editions since the understanding of oral health is always evolving especially in fragile settings like Yemen.
Funding: None
Conflicts of Interest:
The authors declare that they have no conflicts of interest.
Acknowledgments:
The authors acknowledge the support of the University of Aden, the University of Hodeidah. They are grateful to the WHO and IARC for providing such valuable resources. And, of course sincere gratitude to the patients and community members across Yemen who shared their stories with us. Their openness means so much.
REFERENCES
[1] United Nations Development Programme. Yemen: Socioeconomic assessment 2023. New York: UNDP; 2023. https://www.undp.org/yemen/publications/yemen-socioeconomic-assessment-2023
[2] Alhajj WA, AlHaj NJ, Basmail FS, Saleh RA. Prevalence of periodontal diseases and correlations with risk factors among a sample of Yemeni people: cross-sectional study. Braz Dent Sci. 2026;29:e4747. https://doi.org/10.4322/bds.2026.e4747
[3] Al-Sharabi AK, Shuga-Aldin H, Ghandour I, Al-Hebshi NN. Qat chewing as an independent risk factor for periodontitis: a cross-sectional study. Int J Dent. 2013;2013:317640. https://doi.org/10.1155/2013/317640
[4] Kassab A, Al Moustafa AE. Role of Qat Chewing and Mate Consumption in Human Oral Carcinogenesis. In: Al Moustafa AE, ed. Development of Oral Cancer. Cham: Springer; 2017:155-168. https://doi.org/10.1007/978-3-319-48054-1_9
[5] Museedi O, et al. Cultural Practices and Oral Cancer Risk in the Middle East: A Systematic Review. 2025. PMID: 40760977. https://pubmed.ncbi.nlm.nih.gov/40760977/
[6] GBD 2019 Oral Disorders Collaborators. Global, regional, and national burden of oral disorders from 1990 to 2019. J Dent Res. 2021;100(13):1445-1455. https://doi.org/10.1177/00220345211047068
[7] World Health Organization. Global strategy on human resources for health: workforce 2030. Geneva: WHO; 2016. https://www.who.int/publications/i/item/9789241511131
[8] Gallagher JE, Carr E, Brocklehurst P. Health workforce for oral health inequity: Opportunity for action. PLoS One. 2024;19(6):e0292549. https://doi.org/10.1371/journal.pone.0292549
[9] World Health Organization. Oral health surveys: basic methods. 5th ed. Geneva: WHO; 2013. https://www.who.int/publications/i/item/9789241548649
[10] Institute of Medicine (US) Committee for the Study of the Future of Public Health. The future of public health. Washington, DC: National Academies Press; 1988. https://doi.org/10.17226/1091
[11] Dahlgren G, Whitehead M. The Dahlgren-Whitehead model of health determinants: 30 years on. Copenhagen: WHO Regional Office for Europe; 2021. https://www.who.int/europe/publications/i/item/9789289058735
[12] Last JM. A dictionary of epidemiology. 4th ed. Oxford: Oxford University Press; 2001. https://doi.org/10.1093/acref/9780195314496.001.0001
[13] Rothman KJ, Greenland S, Lash TL. Modern epidemiology. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2008. https://www.wolterskluwer.com/en/solutions/ovid/modern-epidemiology-885
[14] Caton JG, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions. J Periodontol. 2018;89(Suppl 1):S1-S8. https://doi.org/10.1002/JPER.18-0157
[15] Fejerskov O, Nyvad B, Kidd E, editors. Dental caries: the disease and its clinical management. 3rd ed. Oxford: Wiley-Blackwell; 2015. https://doi.org/10.1002/9781118935826
[16] Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007;369(9555):51-59. https://doi.org/10.1016/S0140-6736(07)60031-2
[17] World Health Organization. Guideline: sugars intake for adults and children. Geneva: WHO; 2017. https://www.who.int/publications/i/item/9789241549028
[18] Alshamrani KK, AlDhelai TA, Ibrahim RM, Almuallim AM, Alhumaidi AM, Baggash TA, Al Moaleem MM, Shiryan N, Al Makramani B, Qasem AM. Early Primary Molar Loss and Associated Factors among Institutionalized Orphans in Yemen. The Open Dentistry Journal. 2025 Jun 27;19(1).https://opendentistryjournal.com/VOLUME/19/ELOCATOR/e18742106387163/FULLTEXT/
[19] Hassan NA, et al. Qat chewing and oral potentially malignant disorders: A systematic review. J Oral Pathol Med. 2019;48(8):668-675. https://doi.org/10.1111/jop.12923
[20] Ali AA. Histopathologic changes in oral mucosa of Yemenis addicted to water-pipe and cigarette smoking in addition to takhzeen al-qat. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(3):e55-e59. https://doi.org/10.1016/j.tripleo.2006.07.011
[21] International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans: khat. Lyon: IARC; 1985. https://publications.iarc.fr/Book-And-Report-Series/Iarc-Monographs-On-The-Identification-Of-Carcinogenic-Hazards-To-Humans/Khat-1985
[22] International Agency for Research on Cancer. Betel-quid and areca-nut chewing and some areca-nut-derived nitrosamines. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Vol. 85. Lyon: IARC; 2004. https://publications.iarc.fr/100
[23] Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249. https://doi.org/10.3322/caac.21660
[24] Mossey PA, Modell B. Epidemiology of oral clefts 2012. Cleft Palate Craniofac J. 2012;49(6):1-13. https://doi.org/10.1597/11-052
[25] Balint EE, Falkay G, Balint GA. Khat – a controversial plant. Wien Klin Wochenschr. 2009;121(19-20):604-614. https://doi.org/10.1007/s00508-009-1259-7
[26] World Health Organization. Waterpipe tobacco smoking: health effects, research needs and recommended actions for regulators. Geneva: WHO; 2015. https://www.who.int/tobacco/publications/prod_regulation/waterpipe-tobacco-smoking/en/
[27] El-Zaatari ZM, Chami HA, Zaatari GS. Health effects of waterpipe (hookah) smoking: A systematic review. JAMA Intern Med. 2015;175(4):535-545. https://doi.org/10.1001/jamainternmed.2014.8356
[28] Scheifele C, Nassar A, Reichart PA. Prevalence of oral cancer and potentially malignant lesions among shammah users in Yemen. Oral Oncol. 2007;43(1):42-50. https://doi.org/10.1016/j.oraloncology.2005.12.013
[29] Al-Maweri SA, Halboub E, Al-Sufyani G, et al. Is vitamin D deficiency a risk factor for recurrent aphthous stomatitis? A systematic review and meta-analysis. Oral Dis. 2020;26(6):1116-1123. https://doi.org/10.1111/odi.13294
[30] Al-Akwa AA, et al. Dental caries prevalence and its association with fluoride level in drinking water in Sana’a, Yemen. Eur J Dent. 2018;12(1):15-20. https://doi.org/10.4103/ejd.ejd_27_17
[31] United Nations High Commissioner for Refugees. Oral health in humanitarian settings: a needs assessment. Geneva: UNHCR; 2022. https://www.unhcr.org/media/oral-health-humanitarian-settings-needs-assessment
[32] World Health Organization. Oral health in ageing populations. Geneva: WHO; 2015. https://www.who.int/publications/i/item/WHO-NMH-PND-15.1
[33] Hennekens CH, Buring JE. Epidemiology in medicine. Boston: Little, Brown and Company; 1987. https://www.lww.com/product/9780316356367
[34] Levy PS, Lemeshow S. Sampling of populations: methods and applications. 4th ed. Hoboken: Wiley; 2013. https://doi.org/10.1002/9781118627394
[35] Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. https://doi.org/10.2307/2529310
[36] Centers for Disease Control and Prevention. Epi Info user guide. Atlanta: CDC; 2022. https://www.cdc.gov/epiinfo/index.html
[37] R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2023. https://www.R-project.org/
[38] Ford N, et al. Ethics of research in conflict settings. PLoS Med. 2009;6(2):e1000023. https://doi.org/10.1371/journal.pmed.1000023
[39] World Health Organization. Research in fragile and conflict-affected settings. Geneva: WHO; 2017. https://www.who.int/publications/i/item/9789241513227
[40] National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. The Belmont Report. Washington, DC; 1979. https://www.hhs.gov/ohrp/regulations-and-policy/belmont-report/index.html
[41] World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. https://doi.org/10.1001/jama.2013.281053
[42] Becker MH. The health belief model and personal health behavior. Health Educ Monogr. 1974;2(4):324-473. https://doi.org/10.1177/109019817400200407
[43] Bandura A. Social foundations of thought and action: a social cognitive theory. Englewood Cliffs: Prentice-Hall; 1986. https://www.pearson.com/en-us/subject-catalog/p/Bandura-Social-Foundations-of-Thought-and-Action/P200000001106
[44] Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking. J Consult Clin Psychol. 1983;51(3):390-395. https://doi.org/10.1037/0022-006X.51.3.390
[45] World Health Organization. Ottawa Charter for Health Promotion. Geneva: WHO; 1986. https://www.who.int/teams/health-promotion/enhanced-wellbeing/ottawa-charter
[46] Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2024;(7):CD002279. https://doi.org/10.1002/14651858.CD002279.pub3
[47] World Health Organization. Universal health coverage: Oral health. Fact sheet. Geneva: WHO; 2021. https://www.who.int/news-room/fact-sheets/detail/oral-health
[48] World Health Organization. Framework for action on interprofessional education and collaborative practice. Geneva: WHO; 2010. https://www.who.int/publications/i/item/9789241501460
[49] Binagwaho A, et al. Rwanda’s health system: a post-conflict success story. Lancet. 2014;384(9940):294-305. https://doi.org/10.1016/S0140-6736(14)60426-2
[50] Tulchinsky TH, Varavikova EA. The new public health. 3rd ed. San Diego: Academic Press; 2014. https://doi.org/10.1016/C2012-0-01077-5
[51] World Health Organization. Global oral health action plan 2023-2030. Geneva: WHO; 2023. https://www.who.int/publications/i/item/9789240075326
[52] Al-Rai S, Alyousefy M, Al-Twaili Z, et al. Knowledge, practice, and challenges in the use of stainless steel crowns and the Hall technique among Yemeni general dental practitioners: a cross-sectional study. Front Oral Health. 2025;6:1527355. https://doi.org/10.3389/froh.2025.1527355
[53] Oral lesions and related risk factors in Palestine-Gaza. Philos Ethics Humanit Med. 2025;20:42. https://doi.org/10.1186/s13010-025-00204-z
About the Authors and Their Contributions
All four authors contributed equally in developing the textbook, right from the initial idea, concept and scope, to the target audience definition. On top of that, investigation through systematic collection of peer-reviewed studies from Yemen, WHO reports, and various international literature to back up the work.
Dr. Mahmood Md. Mohsen Al-Sakkaf, MSc, PhD – Genetic epidemiologist at the University of Aden with over 40 years of public health research experience in Yemen. ORCID: https://orcid.org/0009-0001-0921-2208. Conceptualisation, methodology, drafting (Chapters 3-4, 11-13), project administration, corresponding author.
Dr. Sami A. Hosain Al-Sakkaf, MSc, PhD – Oral health specialist and orthodontist at the University of Hodeidah, member of CTMES-HU. ORCID: https://orcid.org/0009-0005-0022-7242. Methodology, drafting (Chapters 1-2, 5-10), clinical insights.
Dr. Akram M. Mohammed Al-Sakkaf, MBChB, MPH – Public health physician, implementation researcher, and WHO-TDR fellow; University of Aden. ORCID: https://orcid.org/0000-0003-4709-4596 . Methodology, drafting (Chapters 17-20), figures, co-administration
Dr. Ahmed A. Abdulrahman Al-Sakkaf, BDS – Dentist and clinical researcher, University of Hodeidah. ORCID: https://orcid.org/0009-0009-9914-6635 . Appendices, case studies, figures.
All authors reviewed and approved the final manuscript