IN A NUTSHELL
Editor's note
 By One Health critical lens of examination, this extremely documented masterful article turns the spotlight on the challenges and threats to health currently being perceived in the Ecuadorian areas of Amazon rainforest and Galapagos islands. At a time when consensus has gained traction that humans, animals, plants, and the whole ecosystems are intimately enmeshed and mutually dependent as for individual and global health, this article strongly recommends that a One Health vision shaping the human policies, strategies and practices should be embraced by all policy leaders and decision makers. As a matter of fact, closer collaboration under One Health umbrella would definitely add strength towards global health security and ecosystems integrity achievements
By One Health critical lens of examination, this extremely documented masterful article turns the spotlight on the challenges and threats to health currently being perceived in the Ecuadorian areas of Amazon rainforest and Galapagos islands. At a time when consensus has gained traction that humans, animals, plants, and the whole ecosystems are intimately enmeshed and mutually dependent as for individual and global health, this article strongly recommends that a One Health vision shaping the human policies, strategies and practices should be embraced by all policy leaders and decision makers. As a matter of fact, closer collaboration under One Health umbrella would definitely add strength towards global health security and ecosystems integrity achievements

By Laura H. Kahn, MD, MPH, MPP
Co-Founder, One Health Initiative
Lessons From Ecuador
A One Health Perspective
A One Health Overview
One Health is the concept that human, animal, plant, environmental, and ecosystem health are linked. It’s a relatively new term but an ancient concept understood by indigenous peoples around the world. In her book Braiding Sweetgrass, Robin Wall Kimmerer, a Professor of Environmental Biology at the State University of New York (SUNY), Syracuse and a Citizen Potawatomi Nation tribal member describes how indigenous peoples consider plants and other animals as ‘kin’ and not as objects to own or exploit. Indigenous peoples value the teachings of their kin—the plants and animals—for their health and well-being.
Western cultures do not emphasize how nature sustains us. But we literally incorporate nature into our bodies every day. From the air we breathe, to the plants and animals we eat, to the water we drink, our health and well-being depend on a healthy planet. The One Health concept acknowledges that we are a part of nature, not superior or separate from it. Unfortunately, our hubris and a sense of invulnerability to nature’s limits jeopardizes our future and the future of all species.
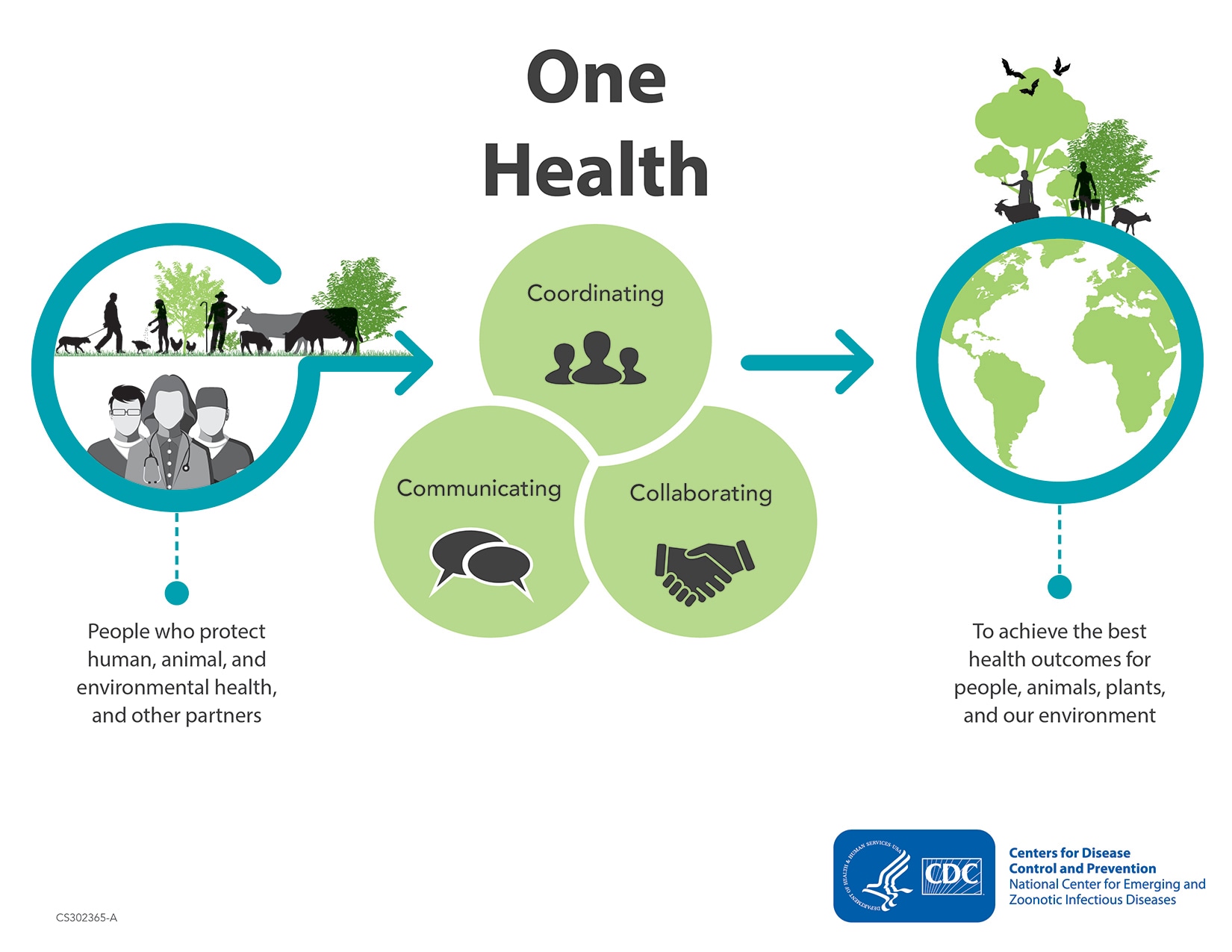
There are many ways to visualize the One Health concept. The Tripartite (World Health Organization, Food and Agriculture Organization, World Organization for Animal Health) and UN Environment Programme depict One Health in a complex way using multiple intersecting circles involving humans, animals, environments, and societies. The US Centers for Disease Control and Prevention (CDC) promotes One Health as intersecting circles involving Coordinating, Communicating, and Collaborating between human, animal, and environmental health professionals.
One Health can also be visualized as a Rubik’s cube representing three intersecting dimensions that form a matrix: a One Health dimension, a Complexity dimension, and a Political, Social, and Economic dimension.

The One Health dimension represents the linkages between humans, animals, plants, environments, and ecosystems. Environments are defined as the abiotic (e.g., soil, water, air) aspects of a defined geographic area. Ecosystems are defined as the biotic (e.g., microbes, flora, fauna) aspects of a defined geographic area. The Complexity dimension provides scale at the microbial/cellular, individual, and population levels. The Political, Social, and Economic dimension can be represented as political borders at local/regional, national, or international levels. This third dimension represents the important social determinants of health and the need to consider health in all policies. Time (e.g., days, months, years) can be a fourth dimension but will not be visualized or discussed in this paper. The intersecting dimensions can be used in whole or in part to provide a systematic, comprehensive, and concise framework to analyze a wide variety of complex, multidisciplinary health-related challenges including those affecting the equitable access to health.
For example, intact forests provide extremely important environmental and ecosystem services such as carbon storage, erosion prevention, climate and water regulation, timber, and non-timber products, as well as food, shelter, and income for indigenous peoples. Forests depend on their environment to supply fresh water for their survival. Andean tropical glaciers deliver essential melt waters to the rainforest and to the indigenous peoples and animals living in the region. Unfortunately, these Andean glaciers are rapidly melting because of climate change, threatening the future of the delicate ecosystems.
In this brief article, the One Health matrix will be used to examine the geographically diverse nation of Ecuador which includes the biodiverse Amazon rainforest and the biosparse Galapagos Islands. With a total area of slightly more than 283 thousand square kilometers, Ecuador is a relatively small nation located on the equator on the west coast of South America. It has a total population of approximately 18 million people. In this paper, the Complexity dimension will focus on the population level.
One Health dimensions of the Amazon Rainforest
While Ecuador possesses only 2 percent of the total Amazon basin, its biodiversity is immense, possessing around 10 percent of Earth’s plants and 8 percent of its animals. Ten out of 14 indigenous tribes in Ecuador live in the tropical rainforest and depend on its natural resources to live. Not surprisingly, the indigenous peoples are important stewards of the land and fight for the forest’s and their own survival. For decades, one of their greatest challenges has been the aggressive presence of large-scale oil drilling that has been causing deforestation and environmental degradation in their territories that threatens their lives. This deforestation taking place in Ecuador is different than in Brazil which has been largely due to intensive agricultural purposes. From 1985 to 2022, Ecuador lost almost 3 million acres of natural land cover, much of it in the Amazon rainforest. Oil extraction has led to multiple spills, emissions, and heavy metal contamination of the region adversely impacting human, animal, and plant health.
Despite their efforts to improve their rights and to protect their ancestral lands by establishing the Confederation of Indigenous Nationalities of Ecuador (CONAIE), the indigenous peoples of Ecuador continue to experience ongoing injustices including serious health threats. Oil drilling is known to contaminate environments and create health risks especially for children. While few quality health studies have been done in the Ecuadorian rainforest, there is evidence to suggest that living near oil production facilities jeopardizes the health of indigenous peoples including increased cancer rates of the colorectum, skin, and kidneys in adults and leukemia in children. One analysis published almost 15 years ago found that indigenous populations had a 30 percent higher mortality rate and a 63 percent higher all-cause morbidity rate compared to non-indigenous colonists living and working in nearby areas. The indigenous peoples particularly suffered from chronic as well as gastrointestinal and vector borne diseases. Many seek traditional medicine from shamans rather than care from Western clinics and hospitals. The Jambi Huasi clinic is attempting to integrate both traditional and Western medicine to meet the cultural demands and health needs of the indigenous peoples.
Data on wildlife health in the Ecuadorian Amazon rainforest is limited. The Wildlife Conservation Society (WCS) has been conducting conservation-based research on wildlife in South America including the Llanganates–Yasuni landscape in Ecuador. A search of the WCS publications database on “Ecuador” yielded 40 unique records, ranging in dates from 2005 to 2020. The publications included census studies of Andean condors, bears, primates, mammals, and birds as well as identifying conservation threats to wildlife such as trafficking and other human activities.
While it’s illegal to possess, buy, or sell wildlife in Ecuador, illegal activity does occur. Private individuals and groups have established centers to protect injured or captured wildlife. For example, in 1993, a small group of individuals established a non-governmental organization (NGO) called amaZOOnico that has received, rehabilitated, and reintroduced thousands of wild animals confiscated from illegal activities. In its 31-year history, it has become one of the largest animal rescue establishments in Ecuador, relying on volunteers and donations for its efforts. Another animal welfare and rehabilitation center established by a private family has been caring for wildlife injured by habitat destruction and illegal trapping for 18 years.
Several non-government organizations exist to protect the Amazon rainforest, although not necessarily only in Ecuador. For example, the Rainforest Alliance fights deforestation and climate change and works to improve the human rights of the indigenous peoples. The Amazon Conservation Team works to protect the rainforest and the indigenous peoples living there, and Amazon Conservation is another one. Like the indigenous peoples of the Amazon, their efforts are in conflict with financial interests.
In August 2023, eight Amazonian nations met and agreed to create an alliance to protect the Amazon rainforest. Unfortunately, they could not agree on a common goal to end deforestation. Instead, they decided to let each nation develop its own deforestation and conservation goals. They agreed that indigenous people’s rights should be considered as well.
One Health dimensions of the Galapagos Islands
In contrast to the Amazon rainforest, the Galapagos Islands are an isolated volcanic archipelago located about 1000 kilometers off the Ecuadorian coast. Discovered in 1535, the islands remained largely uninhabited because of the paucity of fresh water and the dry, inhospitable environment. In the 1920s, Europeans and North Americans began settling there. Today, four (i.e., Santa Cruz, San Cristobal, Isabela, and Floreana) of the 19 largest islands are inhabited by approximately 25-30,000 year-round residents. The population has been growing at a rate of about 6.4 percent per year, but these inhabited areas constitute only about 3 percent of the total area of the islands. In 1959, ninety-seven percent of the islands were designated as a national park which is visited by 170,000-220,000 tourists each year.
The Galapagos Islands were made famous by Charles Darwin’s 1835 visit on board the HMS Beagle which inspired him to develop his theory of “natural selection.” Because the islands are so remote, most species arrived either by flying, being blown by wind, swimming, or floating on a raft. As a result, the wildlife populations on the islands are unique. There are very few native mammals, no native amphibians, a variety of terrestrial and marine birds, and many reptiles. Plant seeds arrived by the wind, or if saltwater tolerant, by sea. The sparce biodiversity created open ecosystem niches that facilitated species to evolve to fill them.
Humans introduced invasive species such as rats to the islands. For example, in the 17th or 18th centuries, the black rat (Rattus rattus) was introduced by whalers and/or pirates. In the 1980s, the brown rat (Rattus norvegicus) was introduced to several islands. Rodents disrupted the delicate ecosystems, and rodent eradication programs have been ongoing.
The people who live in the Galapagos Islands reportedly depend upon imported food for their sustenance and have some of the highest rates of obesity, diabetes, and other chronic diseases in Ecuador. One study published in 2020 found that poor water quality and unhealthy diets consisting of primarily highly processed food contributed to the high disease burden even though the standard of living on the islands compared to the mainland was relatively high. Contaminated tap water led to a reliance on bottled water and sweetened beverages. The authors concluded that rapid population growth, expanding urbanization, food and water insecurity, and tourism contributed to the disease burden.
In June 2022, the Galapagos Science Center (GSC) hosted the World Summit on Island Sustainability on San Cristobal Island. While “One Health” wasn’t the title of the summit, the agenda covered the islands’ ecosystems, environments, animals, and humans. However, Dr. Enrique Teran, a professor at the University San Francisco de Quito, presented his research titled, “One Health Approach to Understanding Human Health on Galapagos Island.” In 2014, he conducted a hospital survey on San Cristobal Island and found that 30 percent of the population was diagnosed with gastrointestinal infections, and many also suffered with urinary tract infections. Poor water quality contaminated with coliforms was a major contributing factor to the infections. Another contributing factor was low socioeconomic status and the ownership of companion animals sick with parasitic infections. In 2019, he found that almost 31 percent of the residents owning companion animals reported that the animals received regular veterinary care, but around 13 percent of the animals had been recently ill. Risk of parasitic illness was higher for humans of lower socioeconomic status (SES) with sick companion animals compared to those with higher SES.
Wildlife and ecosystem health in the Galapagos Islands receive extensive attention and study given the global interest in the islands. For example, since 2016, the GSC has been hosting annual international summits for scientists to share their research on island conservation efforts, the restoration of Galapagos Island marine and terrestrial ecosystems, and the socio-economic issues and health of the island’s human population. The World Wildlife Service (WWS) established a Galapagos Animal Doctors project to treat both wild and domestic animals living on the islands. The Galapagos Conservancy is a U.S. based non-profit organization dedicated to protecting and restoring the Galapagos Islands.
One Health Lessons
From a One Health perspective, human health relies on sanitation and hygiene as well as on healthy animals, plants, environments, and ecosystems. But the indigenous peoples of Ecuador live without sanitation or clean water, and many get sick and die from waterborne diseases. In the Galapagos Islands, only the affluent can afford bottled water.
In Ecuador, the lessons from the Industrial Revolution on the importance of sanitation, clean water, and health are slowly being learned. While the situation has improved over the past decade, the availability of quality drinking water and coverage of sanitation services remains insufficient for the public’s needs particularly in rural areas. In general, wastewater treatment is virtually nonexistent in South America. Most wastewater is dumped into rivers and oceans leading to environmental and ecosystem contamination as well as contributing to water-borne diseases. The indigenous peoples of Ecuador had the highest burden of getting sick and dying from waterborne diseases compared to other ethnic groups in the country.
Unlike the Galapagos Islands which are stringently protected, the Amazon rainforest in Ecuador is not despite having parts of it designated as a UNESCO Biosphere Reserve. The challenge is to convince the political leaders that having an intact rainforest and healthy indigenous peoples is economically beneficial for the country.
Efforts such as the Natural Capital Project seek to quantify the economic value of intact ecosystems. For example, Ecuador is one of the countries working with the Natural Capital Project and the Inter-American Development Bank to design and inform finance and policy decisions. However, surpassing the income generated from oil reserves that would allow the rainforest to remain intact would be a challenge. From a One Health perspective, the world’s leaders should make the health of the rainforest and its indigenous caretakers a priority for the future of humanity and for all other species on the planet.
Addendum
A Brief Historical Aside: Political leaders must be convinced that improving health is beneficial for their nation’s economy. There is historical precedence for this observation. The French Revolution in the late 18th century created fertile ground for French pioneers such as Drs. Louis-Rene Villerme, a pioneer in social epidemiology, and Alexandre Parent-Duchatelet, a leader in the French hygienic movement to improve health. But it wasn’t until Jeremy Bentham, a British social reformer, lawyer, and poor relief advocate, who helped pass a set of “Poor Laws” through Parliament, that actual efforts began to help the working class and poor. Edwin Chadwick, an investigative journalist and lawyer, was hired by Bentham to enquire into the effectiveness of the poor laws.
Bottom line: The poor laws did nothing
Chadwick’s investigation led to the publication of The Report from the Poor Law Commissioners on an Inquiry into the Sanitary Conditions of the Laboring Population of Great Britain. This famous report detailed the wretched environmental and social conditions of Britain’s working class and poor during the beginning of the Industrial Revolution. People lived in slums without sanitation, clean water, pure air, or healthy food. Diseases were rampant. The report planted the seeds for a nascent public health movement. However, only after a deadly cholera epidemic in 1848 did advocacy efforts intensify leading to Parliament to approve a Public Health Act that established a General Board of Health, but it had limited powers and no money. Over the next 50 years, the law was amended to give more power to local boards of health. Ultimately, the political leaders had to be convinced that having healthy workers living in healthy environments benefited the economy. Efforts to improve the equitable access to health for poor, working class, and indigenous peoples, must take this political reality into consideration.












{kind=link}